
Page 19 - 2023 SMOG Digital
P. 19
Trauma
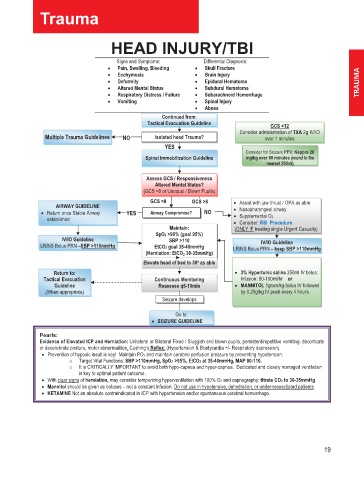
HEAD INJURY/TBI
Signs and Symptoms: Differential Diagnosis:
• Pain, Swelling, Bleeding • Skull Fracture
• Ecchymosis • Brain Injury
• Deformity • Epidural Hematoma
• Altered Mental Status • Subdural Hematoma
• Respiratory Distress / Failure • Subarachnoid Hemorrhage
• Vomiting • Spinal Injury
• Abuse
Continued from:
Tactical Evacuation Guideline GCS <12
Consider administration of TXA 2g IV/IO
Multiple Trauma Guidelines NO Isolated head Trauma? over 1 minutes
YES
Consider for Seizure PPX: Keppra 20
Spinal Immobilization Guideline mg/kg over 60 minutes (round to the e
h
t
r
o
d
(
o
t
n
u
e
n nearest 250ml) l )
s
t
5
a
m
r
2
e
0
Assess GCS / Responsiveness
Altered Mental Status?
(GCS <8 or Unequal / Blown Pupils)
GCS <8 GCS >8 • Assist with jaw thrust / OPA as able
AIRWAY GUIDELINE
• Return once Stable Airway YES Airway Compromise? NO • Nasopharyngeal airway
established • Supplemental O2
• Consider: RSI Procedure
Maintain: (ONLY IF treating single Urgent Casualty)
Sp pO2 >90% (goal 95%)
IV/IO Guideline SBP >110
IV/IO Guideline
LR/NS Bolus PRN –SBP >110mmHg Et tCO2 goal 35-40mmHg LR/NS Bolus PRN – keep SBP >110mmHg
(Herniation: Et tCO 2 30-35mmHg)
Elevate head of bed to 30 0 as able
Return to: • 3% Hypertonic saline 250ml IV bolus:
Tactical Evacuation Continuous Monitoring Infusion: 50-100ml/hr or
Guideline Reassess q5-10min • MANNITOL 1gram/kg bolus IV followed
(When appropriate) by 0.25g/kg IV push every 4 hours.
Seizure develops
Go to:
• SEIZURE GUIDELINE
Pearls:
Evidence of Elevated ICP and Herniation: Unilateral or Bilateral Fixed / Sluggish and blown pupils, persistent/repetitive vomiting, decorticate
or decerebrate posture, motor abnormalities, Cushing’s Reflex: (Hypertension & Bradycardia +/- Respiratory depression)
• Prevention of hypoxic insult is key! Maintain PO2 and maintain cerebral perfusion pressure by preventing hypotension.
o Target Vital Functions: SBP >110mmHg, Sp pO2 >95%, EttCO2 at 35-40mmHg, MAP 80-110.
o It is CRITICALLY IMPORTANT to avoid both hypo-capnea and hyper-capnea. Dedicated and closely managed ventilation
is key to optimal patient outcome.
• With clear signs of herniation, may consider temporizing hyperventilation with 100% O2 and capnography: titrate CO2 to 30-35mmHg.
• Mannitol should be given as boluses – not a constant infusion. Do not use in hypotensive, dehydration, or under-resuscitated patients
• KETAMINE Not an absolute contraindicated in ICP with hypertension and/or spontaneous cerebral hemorrhage.
19