
Page 63 - 2023 SMOG Digital
P. 63
Environmental
Snake Envenomation
Management: General Principles
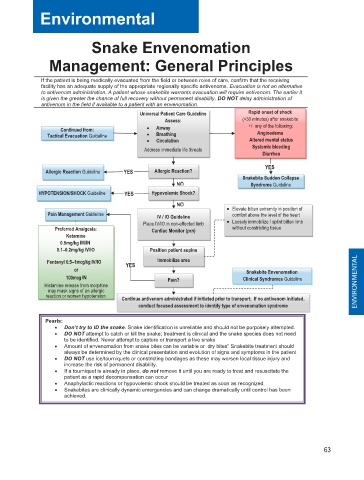
If the patient is being medically evacuated from the field or between roles of care, confirm that the receiving
facility has an adequate supply of the appropriate regionally specific antivenoms. Evacuation is not an alternative
to antivenom administration. A patient whose snakebite warrants evacuation will require antivenom. The earlier it
is given the greater the chance of full recovery without permanent disability. DO NOT delay administration of
antivenom in the field if available to a patient with an envenomation. Rapid onset of shock
Universal Patient Care Guideline
Assess: (<30 minutes) after snakebite
Continued from: • Airway +/- any of the following:
Angioedema
Tactical Evacuation Guideline • Breathing
• Circulation Altered mental status
Address immediate life threats Systemic bleeding
Diarrhea
YES
Allergic Reaction Guideline YES Allergic Reaction?
Snakebite Sudden Collapse
NO Syndrome Guideline
HYPOTENSION/SHOCK Guideline YES Hypovolemic Shock?
NO • Elevate bitten extremity in position of
Pain Management Guideline IV / IO Guideline comfort above the level of the heart
Place IV/IO in non-effected limb • Loosely immobilize / splint bitten limb
Preferred Analgesia: Cardiac Monitor (prn) without constricting tissue
Ketamine
0.5mg/kg IM/IN
0.1– –0.2mg/kg IV/IO Position patient supine
Fentanyl 0 0.5–1mcg/kg IV/IO YES Immobilize area
–
5
m
1
c
g
k
g
.
/
o or r Snakebite Envenomation
g
0
1 100mcg IN Pain? Clinical Syndromes Guideline
0
c
m
Histamine release from morphine ENVIRONMENTAL
may mask signs of an allergic
reaction or worsen hypotension. Continue antivenom administrated if initiated prior to transport. If no antivenom initiated,
conduct focused assessment to identify type of envenomation syndrome
Pearls:
• Don’t try to ID the snake. Snake identification is unreliable and should not be purposely attempted.
• DO NOT attempt to catch or kill the snake; treatment is clinical and the snake species does not need
to be identified. Never attempt to capture or transport a live snake
• Amount of envenomation from snake bites can be variable or dry bites” Snakebite treatment should
always be determined by the clinical presentation and evolution of signs and symptoms in the patient
• DO NOT use ice/tourniquets or constricting bandages as these may worsen local tissue injury and
increase the risk of permanent disability.
• If a tourniquet is already in place, do not remove it until you are ready to treat and resuscitate the
patient as a rapid decompensation can occur
• Anaphylactic reactions or hypovolemic shock should be treated as soon as recognized.
• Snakebites are clinically dynamic emergencies and can change dramatically until control has been
achieved.
63