
Page 58 - 2023 SMOG Digital
P. 58
Cardiac
HYPERTENSION
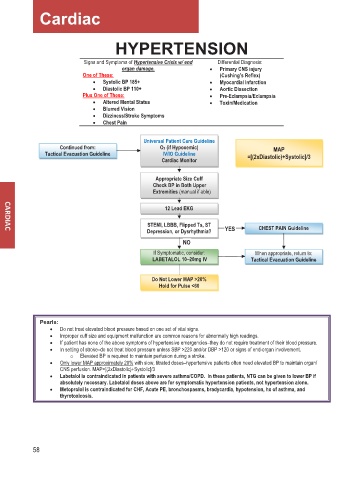
Signs and Symptoms of Hypertensive Crisis w/ end Differential Diagnosis:
organ damage. • Primary CNS injury
One of These: (Cushing’s Reflex)
• Systolic BP 185+ • Myocardial Infarction
• Diastolic BP 110+ • Aortic Dissection
Plus One of These: • Pre-Eclampsia/Eclampsia
• Altered Mental Status • Toxin/Medication
• Blurred Vision
• Dizziness/Stroke Symptoms
• Chest Pain
Universal Patient Care Guideline
Continued from: O2 (if Hypoxemic) MAP
Tactical Evacuation Guideline IV/IO Guideline
Cardiac Monitor =[(2xDiastolic)+Systolic]/3
Appropriate Size Cuff
Check BP in Both Upper
Extremities (manual if able)
12 Lead EKG
STEMI, LBBB, Flipped Ts, ST CHEST PAIN Guideline
Depression, or Dysrhythmia? YES
NO
If Symptomatic, consider: When appropriate, return to:
LABETALOL 10––20mg IV Tactical Evacuation Guideline
Do Not Lower MAP >20%
Hold for Pulse <60
Pearls:
• Do not treat elevated blood pressure based on one set of vital signs.
• Improper cuff size and equipment malfunction are common reasons for abnormally high readings.
• If patient has none of the above symptoms of hypertensive emergencies–they do not require treatment of their blood pressure.
• In setting of stroke–do not treat blood pressure unless SBP >220 and/or DBP >120 or signs of end-organ involvement.
o Elevated BP is required to maintain perfusion during a stroke.
• Only lower MAP approximately 20% with slow, titrated doses–hypertensive patients often need elevated BP to maintain organ/
CNS perfusion. MAP=[(2xDiastolic)+Systolic]/3
• Labetalol is contraindicated in patients with severe asthma/COPD. In these patients, NTG can be given to lower BP if
absolutely necessary. Labetalol doses above are for symptomatic hypertension patients, not hypertension alone.
• Metoprolol is contraindicated for CHF, Acute PE, bronchospasms, bradycardia, hypotension, hx of asthma, and
thyrotoxicosis.
58