
Page 53 - 2023 SMOG Digital
P. 53
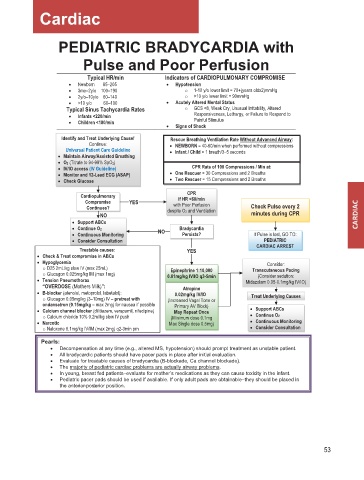
Cardiac
PEDIATRIC BRADYCARDIA with
Pulse and Poor Perfusion
Typical HR/min Indicators of CARDIOPULMONARY COMPROMISE
• Newborn 85–205 • Hypotension
• 3mo–2y/o 100–190 o 1-10 y/o lower limit = 70+(years oldx2)mmHg
• 2y/o–10y/o 60–140 o >10 y/o lower limit = 90mmHg
• >10 y/o 60–100 • Acutely Altered Mental Status
Typical Sinus Tachycardia Rates o GCS <8, Weak Cry, Unusual Irritability, Altered
• Infants <220/min Responsiveness, Lethargy, or Failure to Respond to
• Children <180/min Painful Stimulus
• Signs of Shock
Identify and Treat Underlying Cause! Rescue Breathing Ventilation Rate Without Advanced Airway:
Continue: • NEWBORN = 40-60/min when performed without compressions
Universal Patient Care Guideline • Infant / Child = 1 breath/3–5 seconds
• Maintain Airway/Assisted Breathing
• O2 (Titrate to 94-99% SpO2)
• IV/IO access (IV Guideline) CPR Rate of 100 Compressions / Min at:
• Monitor and 12-Lead ECG (ASAP) • One Rescuer = 30 Compressions and 2 Breaths
• Check Glucose • Two Rescuer = 15 Compressions and 2 Breaths
CPR
Cardiopulmonary if HR <60/min
Compromise YES with Poor Perfusion
Continues? despite O2 and Ventilation Check Pulse every 2
NO minutes during CPR
• Support ABCs
• Continue O2 NO Bradycardia
• Continuous Monitoring Persists? If Pulse is lost, GO TO:
• Consider Consultation PEDIATRIC
Treatable causes: YES CARDIAC ARREST
• Check & Treat compromise in ABCs
• Hypoglycemia Consider:
o D25 2mL/kg slow IV (max 25mL) Epinephrine 1:10,000 Transcutaneous Pacing
o Glucagon 0.025mg/kg IM (max 1mg) 0.01mg/kg IV/IO q3-5min (Consider sedation:
• Tension Pneumothorax Midazolam 0.05-0.1mg/kg IV/IO)
“OVERDOSE (Mothers Milk)”: Atropine
• B-blocker (atenolol, metoprolol, labetalol): 0.02mg/kg IV/IO
o Glucagon 0.05mg/kg (3–10mg) IV – pretreat with (Increased Vagal Tone or Treat Underlying Causes
ondansetron (0.15mg/kg – max 2mg) for nausea if possible Primary AV Block)
• Calcium channel blocker (dilitiazem, verapamil, nifedipine) May Repeat Once • Support ABCs
o Calcium chloride 10% 0.2ml/kg slow IV push (Minimum dose 0.1mg • Continue O2
• Narcotic Max Single dose 0.5mg) • Continuous Monitoring
o Naloxone 0.1mg/kg IV/IM (max 2mg) q2-3min prn • Consider Consultation
Pearls:
• Decompensation at any time (e.g., altered MS, hypotension) should prompt treatment as unstable patient.
• All bradycardic patients should have pacer pads in place after initial evaluation.
• Evaluate for treatable causes of bradycardia (B-blockade, Ca channel blockade).
• The majority of pediatric cardiac problems are actually airway problems.
• In young, breast fed patients–evaluate for mother’s medications as they can cause toxicity in the infant.
• Pediatric pacer pads should be used if available. If only adult pads are obtainable–they should be placed in
the anterior-posterior position.
53