
Page 49 - 2023 SMOG Digital
P. 49
Cardiac
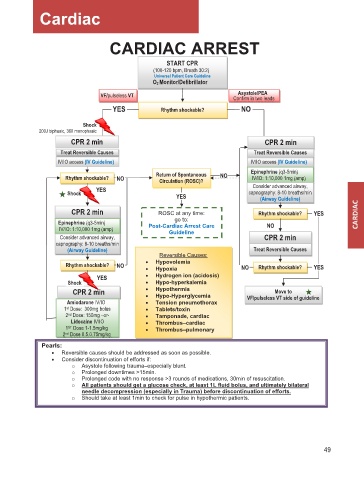
CARDIAC ARREST
START CPR
(100-120 bpm, Breath 30:2)
Universal Patient Care Guideline
O2 Monitor/Defibrillator
Asystole/PEA
VF/pulseless VT Confirm in two leads
YES Rhythm shockable? NO
Shock
200J biphasic, 360 monophasic
CPR 2 min CPR 2 min
Treat Reversible Causes Treat Reversible Causes
IV/IO access (IV Guideline) IV/IO access (IV Guideline)
Return of Spontaneous NO Epinephrine (q3-5min)
Rhythm shockable? NO Circulation (ROSC)? IV/IO: 1:10,000 1mg (amp)
YES Consider advanced airway,
Shock capnography: 8-10 breaths/min
YES (Airway Guideline)
CPR 2 min ROSC at any time: Rhythm shockable? YES
Epinephrine (q3-5min) go to: NO
IV/IO: 1:10,000 1mg (amp) Post-Cardiac Arrest Care
Guideline
Consider advanced airway, CPR 2 min
capnography: 8-10 breaths/min
(Airway Guideline) Treat Reversible Causes
Reversible Causes:
Rhythm shockable? NO • • Hypovolemia NO Rhythm shockable? YES
Hypoxia
YES • Hydrogen ion (acidosis)
Shock • Hypo-hyperkalemia
CPR 2 min • • Hypothermia Move to
Hypo-Hyperglycemia
Amiodarone IV/IO • Tension pneumothorax VF/pulseless VT side of guideline
1 st Dose: 300mg bolus • Tablets/toxin
2 nd Dose: 150mg –or- • Tamponade, cardiac
Lidocaine IV/IO • Thrombus–cardiac
1 ST Dose 1-1.5mg/kg • Thrombus–pulmonary
2 nd Dose 0.5.0.75mg/kg
Pearls:
• Reversible causes should be addressed as soon as possible.
• Consider discontinuation of efforts if:
o Asystole following trauma–especially blunt.
o Prolonged downtimes >15min.
o Prolonged code with no response >3 rounds of medications, 30min of resuscitation.
o All patients should get a glucose check, at least 1L fluid bolus, and ultimately bilateral
needle decompression (especially in Trauma) before discontinuation of efforts.
o Should take at least 1min to check for pulse in hypothermic patients.
49