
Page 48 - 2023 SMOG Digital
P. 48
Cardiac
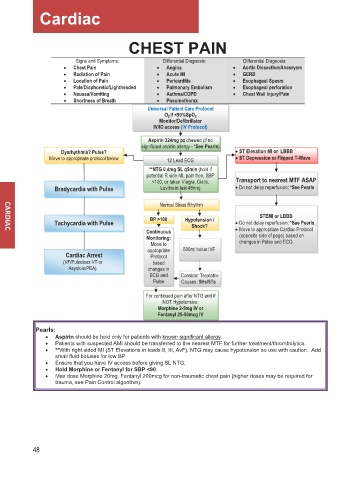
CHEST PAIN
Signs and Symptoms: Differential Diagnosis: Differential Diagnosis:
• Chest Pain • Angina • Aortic Dissection/Aneurysm
• Radiation of Pain • Acute MI • GERD
• Location of Pain • Pericarditis • Esophageal Spasm
• Pale/Diaphoretic/Lightheaded • Pulmonary Embolism • Esophageal perforation
• Nausea/Vomiting • Asthma/COPD • Chest Wall Injury/Pain
• Shortness of Breath • Pneumothorax
Universal Pati en t Care Protocol
O O 2 If <90%SpO 2
2
Monitor/Defibrillator
IV/IO access (IV Protocol)
o
Aspirin 324mg ppo chewed (if no
significant aspirin allergy - *See Pearls)
Dysrhythmia? Pulse? • ST Elevation MI or LBBB
Move to appropriate protocol below 12 Lead ECG • ST Depression or Flipped T-Wave
**NTG 0.4mg SL q5min (hold if
potential R side MI, pain free, SBP
<100, or taken Viagra, Cialis, Transport to nearest MTF ASAP
Bradycardia with Pulse Levitra in last 48hrs) • Do not delay reperfusion: *See Pearls
Normal Sinus Rhythm
STEMI or LBBB
Tachycardia with Pulse BP >100 Hypotension / • Do not delay reperfusion: *See Pearls.
Shock?
Continuous • Move to appropriate Cardiac Protocol
Monitoring: (opposite side of page) based on
Move to changes in Pulse and ECG.
appropriate 500ml bolus IVF
Cardiac Arrest Protocol
(VF/Pulseless VT or based
Asystole/PEA) changes in
ECG and Consider Treatable
Pulse Causes: 5Hs/5Ts
For continued pain after NTG and if
NOT Hypotensive:
Morphine 2-5mg IV or
Fentanyl 25-50mcg IV
Pearls:
• Aspirin should be held only for patients with known significant allergy.
• Patients with suspected AMI should be transferred to the nearest MTF for further treatment/thrombolytics.
• **With right sided MI (ST Elevations in leads II, III, AvF), NTG may cause hypotension so use with caution. Add
small fluid boluses for low BP.
• Ensure that you have IV access before giving SL NTG.
• Hold Morphine or Fentanyl for SBP <90.
• Max dose Morphine 20mg, Fentanyl 200mcg for non-traumatic chest pain (higher doses may be required for
trauma, see Pain Control algorithm).
48