
Page 59 - 2023 SMOG Digital
P. 59
Environmental
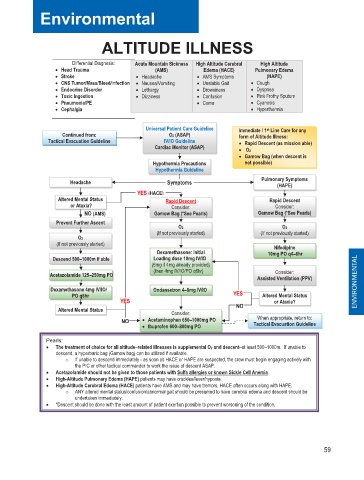
ALTITUDE ILLNESS
Differential Diagnosis: Acute Mountain Sickness High Altitude Cerebral High Altitude
• Head Trauma (AMS) Edema (HACE) Pulmonary Edema
• Stroke • Headache • AMS Symptoms (HAPE)
I
n
• CNS Tumor/Mass/Bleed/Infection • Nausea/Vomiting • Unstable Gait • Cough
• Endocrine Disorder • Lethargy • Drowsiness • Dyspnea
• Toxic Ingestion • Dizziness • Confusion • Pink Frothy Sputum
• Pneumonia/PE • Coma • Cyanosis
• Cephalgia • Hyperthermia
Universal Patient Care Guideline Immediate / 1 st Line Care for any
Continued from: O2 (ASAP) form of Altitude Illness:
Tactical Evacuation Guideline IV/IO Guideline • Rapid Descent (as mission able)
Cardiac Monitor (ASAP)
• O2
• Gamow Bag (when descent is
Hypothermia Precautions not possible)
Hypothermia Guideline
Pulmonary Symptoms
Headache Symptoms (HAPE)
YES (HACE)
Altered Mental Status Rapid Descent Rapid Descent
or Ataxia? Consider: Consider:
NO (AMS) Gamow Bag (*See Pearls) Gamow Bag (*See Pearls)
Prevent Further Ascent
O2 O2
(If not previously started) (If not previously started)
O2
(If not previously started) Nifedipine
Dexamethasone: Initial 10mg PO q4–6hr
–
Descend 500–1000m if able Loading dose 10mg IV/IO
–
(6mg if 4mg already provided)
Acetazolamide 125–250mg PO (then 4mg IV/IO/PO q6hr) Consider:
–
Assisted Ventilation (PPV) ENVIRONMENTAL
Dexamethasone 4mg IV/IO/ Ondansetron 4–8mg IV/IO
–
PO q6hr YES Altered Mental Status
YES or Ataxia?
Altered Mental Status Consider: NO
When appropriate, return to:
–
NO • Acetaminophen 650–1000mg PO Tactical Evacuation Guideline
• Ibuprofen 600–800mg PO
–
Pearls:
–
• The treatment of choice for all altitude–related illnesses is supplemental O2 and descent–at least 500–1000m. If unable to
descend, a hyperbaric bag (Gamow bag) can be utilized if available.
o If unable to descend immediately - as soon as HACE or HAPE are suspected, the crew must begin engaging actively with
the PIC or other tactical commander to work the issue of descent ASAP.
• Acetazolamide should not be given to those patients with Sulfa allergies or known Sickle Cell Anemia.
• High-Altitude Pulmonary Edema (HAPE) patients may have crackles/fever/hypoxia.
• High-Altitude Cerebral Edema (HACE) patients have AMS and may have tremors, HACE often occurs along with HAPE.
o ANY altered mental status/confusion/abnormal gait should be presumed to have cerebral edema and descent should be
undertaken immediately.
• *Descent should be done with the least amount of patient exertion possible to prevent worsening of the condition.
59