
Page 122 - JSOM Winter 2017
P. 122
fracture (so-called trapdoor fracture). The resultant
traction on the rectus muscle can trigger the oculocar-
diac reflex and result in intractable nausea and vomit-
ing, symptomatic bradycardia, and possibly heart block.
Although this is more common in pediatric patients
(termed “white-eye” blow-out fractures), it is not exclu-
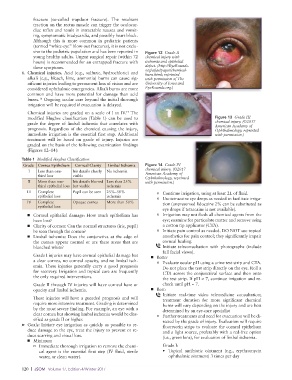
sive to the pediatric population and has been reported in Figure 12 Grade II
young healthy adults. Urgent surgical repair (within 72 chemical injury with
hours) is recommended for an entrapped fracture with ischemia and epithelial
these symptoms. defect. (http://EyeRounds.
6. Chemical injuries. Acid (e.g., sulfuric, hydrochloric) and org/atlas/pages/chemical-
burn.html; reprinted
alkali (e.g., bleach, lime, ammonia) burns can cause sig- with permission of The
nificant injuries leading to permanent loss of vision and are University of Iowa and
considered ophthalmic emergencies. Alkali burns are more EyeRounds.org.)
common and have more potential for damage than acid
burns. Ongoing ocular care beyond the initial thorough
16
irrigation will be required if evacuation is delayed.
17
Chemical injuries are graded on a scale of I to IV. The
modified Hughes classification (Table 1) can be used to Figure 13 Grade III
grade the degree of limbal ischemia that correlates with chemical injury. (©2017
prognosis. Regardless of the chemical causing the injury, American Academy of
Ophthalmology, reprinted
immediate irrigation is the essential first step. Additional with permission.)
treatment will be based on grade of injury. Injuries are
graded on the basis of the following examination findings
(Figures 12–14):
Table 1 Modified Hughes Classification
Grade Cornea Epithelium Corneal Clarity Limbal Ischemia Figure 14 Grade IV
chemical injury. (©2017
I Less than one- Iris details clearly No ischemia
third loss visible American Academy of
Ophthalmology, reprinted
II More than one- Iris details blurred Less than 25% with permission.)
third epithelial loss but visible ischemia
III Complete Pupil can be seen 25%–50% o Continue irrigation, using at least 2L of fluid.
epithelial loss ischemia o Use tetracaine eye drops as needed to facilitate irriga-
IV Complete Opaque cornea More than 50% tion (unpreserved lidocaine 2% can be substituted as
epithelial loss
eye drops if tetracaine is not available).
■ Corneal epithelial damage: How much epithelium has o Irrigation may not flush all chemical agents from the
been lost? eye; examine for particulate matter and remove using
■ Clarity of cornea: Can the normal structures (iris, pupil) a cotton tip applicator (CTA).
be seen through the cornea? o Initiate pain control as needed. DO NOT use topical
■ Limbal ischemia: Does the conjunctiva at the edge of anesthetics for pain control; they significantly impair
the cornea appear normal or are there areas that are corneal healing.
blanched white? Initiate teleconsultation with photographs (include
full facial views).
Grade I injuries may have corneal epithelial damage but ■ Better
a clear cornea, no corneal opacity, and no limbal isch- o Evaluate ocular pH using a urine test strip and CTA.
emia. These injuries generally carry a good prognosis Do not place the test strip directly on the eye. Roll a
for recovery. Irrigation and topical care are frequently CTA across the conjunctival surface and then onto
the only required interventions. the test strip. If pH ≠ 7, continue irrigation and re-
Grade II through IV injuries will have corneal haze or check until pH = 7.
opacity and limbal ischemia. ■ Best:
Initiate real-time video telemedicine consultation;
These injuries will have a guarded prognosis and will treatment duration for more significant chemical
require more intensive treatment. Grading is determined burns will vary depending on the injury and are best
by the most severe finding. For example, an eye with a determined by an eye-care specialist
clear cornea but showing limbal ischemia would be clas- o Further treatments and need for evacuation will be di-
sified as grade II or higher. rected by the grade of injury. Evaluation will require
➤ Goals: Initiate eye irrigation as quickly as possible to re- fluorescein strips to evaluate the corneal epithelium
duce damage to the eye, treat the injury to prevent or re- and a light source, preferably with a red-free option
duce scarring and visual loss. (i.e., green lens), for evaluation of limbal ischemia.
■ Minimum
o Immediate thorough irrigation to remove the chemi- Grade I:
cal agent is the essential first step (IV fluid, sterile • Topical antibiotic ointment (e.g., erythromycin
water, or clean water). ophthalmic ointment) 3 times per day
120 | JSOM Volume 17, Edition 4/Winter 2017