
Page 119 - JSOM Winter 2017
P. 119
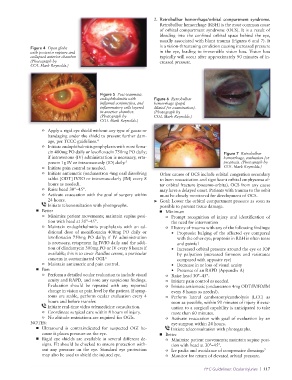
2. Retrobulbar hemorrhage/orbital compartment syndrome.
Retrobulbar hemorrhage (RBH) is the most common cause
of orbital compartment syndrome (OCS). It is a result of
bleeding into the confined orbital space behind the eye,
usually associated with blunt trauma (Figures 6 and 7). It
is a vision-threatening condition causing increased pressure
Figure 4 Open globe
with posterior rupture and in the eye, leading to irreversible vision loss. Vision loss
collapsed anterior chamber. typically will occur after approximately 90 minutes of in-
(Photograph by creased pressure.
COL Mark Reynolds.)
Figure 5 Post-traumatic
endophthalmitis with Figure 6 Retrobulbar
inflamed conjunctiva, and hemorrhage (pupil
inflammatory cells layered dilated for examination).
in anterior chamber. (Photograph by
(Photograph by COL Mark Reynolds.)
COL Mark Reynolds.)
o Apply a rigid eye shield without any type of gauze or
bandaging under the shield to prevent further dam-
age, per TCCC guidelines. 4
o Initiate endophthalmitis prophylaxis with moxifloxa-
cin 400mg PO daily or levofloxacin 750mg PO daily; Figure 7 Retrobulbar
if intravenous (IV) administration is necessary, erta- hemorrhage, evaluation for
penem 1g IV or intraosseously (IO) daily. 5 proptosis. (Photograph by
o Initiate pain control as needed. COL Mark Reynolds.)
o Initiate antiemetic (ondansetron 4mg oral dissolving Other causes of OCS include orbital congestion secondary
tablet [ODT] IV/IO or intramuscularly [IM] every 8 to burn resuscitation and significant orbital emphysema af-
hours as needed). ter orbital fracture (pneumo-orbita). OCS from any cause
o Raise head 30°–45°. may have a delayed onset. Patients with trauma to the orbit
o Activate evacuation with the goal of surgery within must be closely monitored for development of OCS.
24 hours. ➤ Goal: Lower the orbital compartment pressure as soon as
Initiate teleconsultation with photographs. possible to prevent tissue damage.
■ Better ■ Minimum
o Minimize patient movements; maintain supine posi- o Prompt recognition of injury and identification of
tion with head at 30°–45°. the need for intervention
o Maintain endophthalmitis prophylaxis with an ad- o History of trauma with any of the following findings:
ditional dose of moxifloxacin 400mg PO daily or • Proptosis: bulging of the affected eye compared
levofloxacin 750mg PO daily; if IV administration with the other eye; proptosis in RBH is often tense
is necessary, ertapenem 1g IV/IO daily and the addi- and painful
tion of clindamycin 300mg PO or IV every 8 hours if • Increased orbital pressure around the eye or IOP
available; this is to cover Bacillus cereus, a particular by palpation (increased firmness and resistance
concern in contaminated OGI. 6 compared with opposite eye)
o Maintain antiemetic and pain control. • Decrease in or loss of visual acuity
■ Best • Presence of an RAPD (Appendix A)
o Perform a detailed ocular evaluation to include visual o Raise head 30°–45°.
acuity and RAPD, and note any suspicious findings. o Initiate pain control as needed.
Evaluation should be repeated with any reported o Initiate antiemetic (ondansetron 4mg ODT/IV/IO/IM
change in vision or pain level by the patient. If symp- every 8 hours as needed).
toms are stable, perform ocular evaluation every 4 o Perform lateral canthotomy/cantholysis (LCC) as
hours and before transfer. soon as possible, within 90 minutes of injury if evac-
Initiate real-time video telemedicine consultation. uation to a surgical capability is anticipated to take
o Coordinate surgical care within 8 hours of injury. more than 60 minutes.
o No altitude restrictions are required for OGIs. o Activate evacuation with goal of evaluation by an
NOTES: eye surgeon within 24 hours.
■ Ultrasound is contraindicated for suspected OGI be- Initiate teleconsultation with photographs.
cause it places pressure on the eye. ■ Better
■ Rigid eye shields are available in several different de- o Minimize patient movements; maintain supine posi-
signs. Fit should be checked to ensure protection with- tion with head at 30°–45°.
out any pressure on the eye. Standard eye protection o Ice packs and avoidance of compressive dressings 7
may also be used to shield the injured eye. o Monitor for return of elevated orbital pressure.
PFC Guidelines: Ocular Injuries | 117