
Page 184 - 2023 SMOG Digital
P. 184
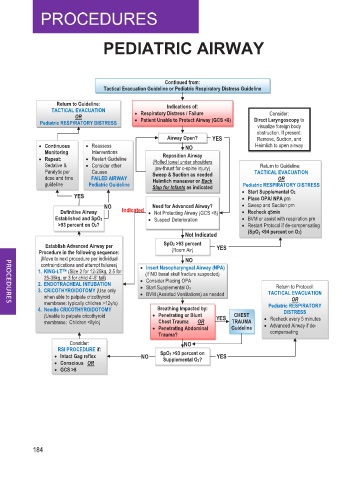
PEDIATRIC AIRWAY
Continued from:
Tactical Evacuation Guideline or Pediatric Respiratory Distress Guideline
Return to Guideline: Indications of:
TACTICAL EVACUATION • Respiratory Distress / Failure
Consider:
OR Direct Laryngoscopy to
Pediatric RESPIRATORY DISTRESS • Patient Unable to Protect Airway (GCS <8) visualize foreign body
obstruction. If present:
Airway Open? YES Remove, Suction, and
• Continuous • Reassess NO Heimlich to open airway
Monitoring Interventions Reposition Airway
• Repeat: • Restart Guideline (Rolled towel under shoulders
Sedative & • Consider other jaw-thrust for c-spine injury) Return to Guideline:
Paralytic per Causes Sweep & Suction as needed TACTICAL EVACUATION
dose and time FAILED AIRWAY Heimlich maneuver or Back OR
guideline Pediatric Guideline Slap for Infants as indicated Pediatric RESPIRATORY DISTRESS
YES • Start Supplemental O2
• Place OPA/ NPA prn
NO Need for Advanced Airway? • Sweep and Suction prn
q
5
m
Definitive Airway Indicated • Not Protecting Airway (GCS <8) • Recheck q5min i n
Established and SpO2 • Suspect Deterioration • BVM or assist with respiration prn
>93 percent on O2? • Restart Protocol if de-compensating
Not Indicated (SpO 2 <94 percent on O2)
Establish Advanced Airway per SpO2 >93 percent YES
Procedure in the following sequence: (Room Air)
(Move to next procedure per individual NO
contraindications and attempt failures) • Insert Nasopharyngeal Airway (NPA)
1. KING-LT™ (Size 2 for 12-25kg, 2.5 for (If NO basal skull fracture suspected)
25-35kg, or 3 for child 4’-5’ tall) • Consider Placing OPA
2. ENDOTRACHEAL INTUBATION Return to Protocol:
3. CRICOTHYROIDOTOMY (Use only • Start Supplemental O2 TACTICAL EVACUATION
when able to palpate cricothyroid • BVM (Assisted Ventilations) as needed OR
membrane: typically children >12y/o) Pediatric RESPIRATORY
4. Needle CRICOTHYROIDOTOMY Breathing Impacted by: DISTRESS
(Unable to palpate cricothyroid • Penetrating or Blunt YES CHEST • Recheck every 5 minutes
membrane: Children <8y/o) Chest Trauma OR TRAUMA • Advanced Airway if de-
• Penetrating Abdominal Guideline
Trauma? compensating
Consider: NO
RSI PROCEDURE if:
• Intact Gag reflex NO SpO2 >93 percent on YES
Supplemental O2?
• Conscious OR
• GCS >8
184