
Page 188 - 2023 SMOG Digital
P. 188
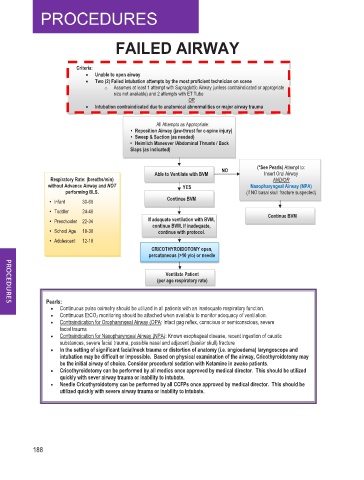
FAILED AIRWAY
Criteria:
• Unable to open airway
• Two (2) Failed intubation attempts by the most proficient technician on scene
o Assumes at least 1 attempt with Supraglottic Airway (unless contraindicated or appropriate
size not available) and 2 attempts with ET Tube
OR
• Intubation contraindicated due to anatomical abnormalities or major airway trauma
All Attempts as Appropriate:
• Reposition Airway (jaw-thrust for c-spine injury)
• Sweep & Suction (as needed)
• Heimlich Maneuver /Abdominal Thrusts / Back
Slaps (as indicated)
NO (*See Pearls) Attempt to:
Able to Ventilate with BVM Insert Oral Airway
p
s
Respiratory Rate: (breaths/min) AND/OR
without Advance Airway and NOT YES Nasopharyngeal Airway (NPA)
performing BLS. (if NO basal skull fracture suspected)
• Infant 30-60 Continue BVM
• Toddler 24-40 Continue BVM
• Preschooler 22-34 If adequate ventilation with BVM,
continue BVM. If inadequate,
• School Age 18-30 continue with protocol.
• Adolescent 12-18
CRICOTHYROIDOTOMY open,
percutaneous (>10 y/o) or needle
Ventilate Patient
(per age respiratory rate)
Pearls:
Continuous pulse oximetry should be utilized in all patients with an inadequate respiratory function.
Continuous EtCO2 monitoring should be attached when available to monitor adequacy of ventilation.
Contraindication for Oropharyngeal Airway (OPA: Intact gag reflex, conscious or semiconscious, severe
facial trauma
Contraindication for Nasopharyngeal Airway (NPA): Known esophageal disease, recent ingestion of caustic
substances, severe facial trauma, possible nasal and adjacent (basilar skull) fracture
In the setting of significant facial/neck trauma or distortion of anatomy (i.e. angioedema) laryngoscope and
intubation may be difficult or impossible. Based on physical examination of the airway, Cricothyroidotomy may
be the initial airway of choice. Consider procedural sedation with Ketamine in awake patients.
Cricothyroidotomy can be performed by all medics once approved by medical director. This should be utilized
quickly with sever airway trauma or inability to intubate.
Needle Cricothyroidotomy can be performed by all CCFPs once approved by medical director. This should be
utilized quickly with severe airway trauma or inability to intubate.
188