
Page 191 - 2023 SMOG Digital
P. 191
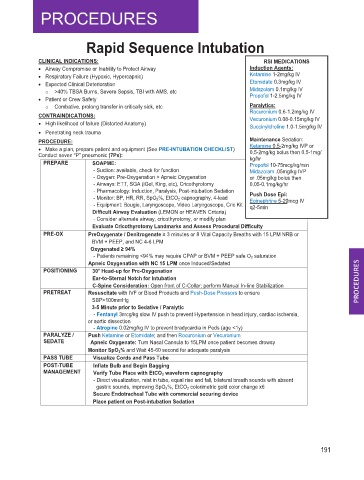
Rapid Sequence Intubation
CLINICAL INDICATIONS: RSI MEDICATIONS
• Airway Compromise or Inability to Protect Airway Induction Agents:
• Respiratory Failure (Hypoxic, Hypercapnic) Ketamine 1-2mg/kg IV
• Expected Clinical Deterioration Etomidate 0.3mg/kg IV
o >40% TBSA Burns, Severe Sepsis, TBI with AMS, etc Midazolam 0.1mg/kg IV
Propofol 1-2.5mg/kg IV
• Patient or Crew Safety
o Combative, prolong transfer in critically sick, etc Paralytics:
Rocuronium 0.6-1.2mg/kg IV
CONTRAINDICATIONS: Vecuronium 0.08-0.15mg/kg IV
• High likelihood of failure (Distorted Anatomy) Succinylcholine 1.0-1.5mg/kg IV
• Penetrating neck trauma
PROCEDURE: Maintenance Sedation:
• Make a plan, prepare patient and equipment (See PRE-INTUBATION CHECKLIST) Ketamine 0.5-2mg/kg IVP or
Conduct seven “P” pneumonic (7Ps): 0.5-2mg/kg bolus then 0.5-1mg/
kg/hr
PREPARE SOAPME: Propofol 10-75mcg/kg/min
- Suction: available, check for function Midazolam .05mg/kg IVP
- Oxygen: Pre-Oxygenation + Apneic Oxygenation or .05mg/kg bolus then
- Airways: ETT, SGA (iGel, King, etc), Cricothyrotomy 0.05-0.1mg/kg/hr
- Pharmacology: Induction, Paralysis, Post-intubation Sedation
- Monitor: BP, HR, RR, SpO 2 %, EtCO 2 capnography, 4-lead Push Dose Epi:
Epinephrine 5-20mcg IV
- Equipment: Bougie, Laryngoscope, Video Laryngoscope, Cric Kit q2-5min
Difficult Airway Evaluation (LEMON or HEAVEN Criteria)
- Consider alternate airway, cricothyrotomy, or modify plan
Evaluate Cricothyrotomy Landmarks and Assess Procedural Difficulty
PRE-OX PreOxygenate / Denitrogenate ≥ 3 minutes or 8 Vital Capacity Breaths with 15 LPM NRB or
BVM + PEEP, and NC 4-6 LPM
Oxygenated ≥ 94%
- Patients remaining <94% may require CPAP or BVM + PEEP safe O 2 saturation
Apneic Oxygenation with NC 15 LPM once Induced/Sedated
POSITIONING 30° Head-up for Pre-Oxygenation
Ear-to-Sternal Notch for Intubation
C-Spine Consideration: Open front of C-Collar; perform Manual In-line Stabilization
PRETREAT Resuscitate with IVF or Blood Products and Push-Dose Pressors to ensure
SBP>100mmHg
3-5 Minute prior to Sedative / Paralytic
- Fentanyl 3mcg/kg slow IV push to prevent Hypertension in head injury, cardiac ischemia,
or aortic dissection
- Atropine 0.02mg/kg IV to prevent bradycardia in Peds (age <1y)
PARALYZE / Push Ketamine or Etomidate; and then Rocuronium or Vecuronium
SEDATE Apneic Oxygenate: Turn Nasal Cannula to 15LPM once patient becomes drowsy
Monitor SpO 2 % and Wait 45-60 second for adequate paralysis
PASS TUBE Visualize Cords and Pass Tube
POST-TUBE Inflate Bulb and Begin Bagging
MANAGEMENT Verify Tube Place with EtCO 2 waveform capnography
- Direct visualization, mist in tube, equal rise and fall, bilateral breath sounds with absent
gastric sounds, improving SpO 2 %, EtCO 2 colorimetric gold color change x6
Secure Endotracheal Tube with commercial securing device
Place patient on Post-intubation Sedation
191