
Page 42 - JSOM Summer 2025
P. 42
arduous process that congests heated environments needed for for symptom resolution or definitive signs of frostbite, such
more severe casualties. This is especially true early in the dis- as blistering or persistent and demarcated skin discoloration.
ease process, when the primary symptom is numbness, without If symptoms improve, the Soldier is returned to duty. If sub-
the blisters, discoloration, or induration associated with more jective symptoms persist, serial neurological examinations are
developed frostbite. Inappropriate disposition and immediate performed. These exams include sensitivity to light touch, hot/
re-exposure to freezing temperatures dramatically worsens the cold sensitivity, and two-point discrimination. If the Soldier
disease and may result in amputation of the affected tissue. Ef- has a normal examination, then they are thought to not have
ficiently differentiating transient post-cold exposure neuropa- a significant frostbite injury and will be able to self-identify
thy or erythema from permanent tissue damage will improve future symptoms of frostbite when re-exposed to the cold.
throughput within the medical treatment facility and rapidly
return Soldiers to duty. In limited initial testing, of the 14 Soldiers who entered the
pathway and were returned to duty, none re-presented later
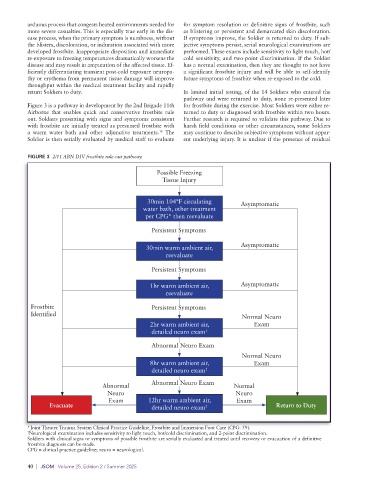
Figure 3 is a pathway in development by the 2nd Brigade 11th for frostbite during the exercise. Most Soldiers were either re-
Airborne that enables quick and conservative frostbite rule turned to duty or diagnosed with frostbite within two hours.
out. Soldiers presenting with signs and symptoms consistent Further research is required to validate this pathway. Due to
with frostbite are initially treated as presumed frostbite with harsh field conditions or other circumstances, some Soldiers
a warm water bath and other adjunctive treatments. The may continue to describe subjective symptoms without appar-
16
Soldier is then serially evaluated by medical staff to evaluate ent underlying injury. It is unclear if the presence of residual
FIGURE 3 2/11 ABN DIV frostbite rule-out pathway.
Possible Freezing
Tissue Injury
30min 104°F circulating Asymptomatic
water bath, other treatment
per CPG* then reevaluate
Persistent Symptoms
30min warm ambient air, Asymptomatic
reevaluate
Persistent Symptoms
1hr warm ambient air, Asymptomatic
reevaluate
Frostbite Persistent Symptoms
Identified Normal Neuro
2hr warm ambient air, Exam
detailed neuro exam †
Abnormal Neuro Exam
Normal Neuro
8hr warm ambient air, Exam
detailed neuro exam †
Abnormal Abnormal Neuro Exam Normal
Neuro Neuro
Exam 12hr warm ambient air, Exam
Evacuate detailed neuro exam † Return to Duty
*Joint Theater Trauma System Clinical Practice Guideline, Frostbite and Immersion Foot Care (CPG: 59).
† Neurological examination includes sensitivity to light touch, hot/cold discrimination, and 2-point discrimination.
Soldiers with clinical signs or symptoms of possible frostbite are serially evaluated and treated until recovery or evacuation of a definitive
frostbite diagnosis can be made.
CPG = clinical practice guideline; neuro = neurological.
40 | JSOM Volume 25, Edition 2 / Summer 2025