
Page 135 - JSOM Spring 2020
P. 135
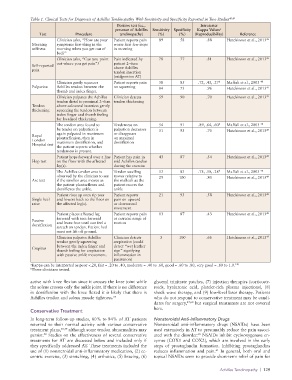
Table 1. Clinical Tests for Diagnosis of Achilles Tendinopathy With Sensitivity and Specificity Reported in Two Studies 48,49
Positive test (i.e., Intratester
presence of Achilles Sensitivity Specificity Kappa Values a
Test Procedure tendinopathy) (%) (%) (Reproducibility) Reference
Clinician asks, “How are your Patient reports pain 89 58 .88 Hutchinson et al., 2013 49
Morning symptoms first thing in the worse first few steps
stiffness morning when you get out of in morning
bed?”
Clinician asks, “Can you point Pain indicated by 78 77 .81 Hutchinson et al., 2013 49
out where you get pain”? patient 2–6cm
Self-reported
pain above Achilles
tendon insertion
(midportion AT)
Clinician gently squeezes Patient reports pain 58 85 .72, .43, .27 b Maffuli et al., 2003 48
Palpation Achilles tendon between the on squeezing 84 73 .96 Hutchinson et al., 2013 49
thumb and index finger.
Clinician palpates the Achilles Clinician detects 59 90 .70 Hutchinson et al., 2013 49
tendon distal to proximal 2–6cm tendon thickening
Tendon above calcaneal insertion gently
thickening squeezing the tendon between
index finger and thumb feeling
for localized thickening.
The tendon area found to Tenderness on 54 91 .89, .64, .60 b Maffuli et al., 2003 48
be tender on palpation is palpation decreases 51 93 .70 Hutchinson et al., 2013 49
again palpated in maximum or disappears
Royal plantarflexion, then in on maximal
London maximum dorsiflexion, and dorsiflexion
Hospital test
the patient reports whether
tenderness is present.
Patient hops forward over a line Patient has pain in 43 87 .54 Hutchinson et al., 2013 49
Hop test on the floor with the affected mid Achilles tendon
leg(s). during the exercise
The Achilles tendon area is Tendon swelling 53 83 .75, .50, .28 b Maffuli et al., 2003 48
observed by the clinician to see moves relative to 25 100 .80 Hutchinson et al., 2013 49
Arc test if the swollen area moves as the malleoli as the
the patient plantarflexes and patient moves the
dorsiflexes the ankle. ankle
Patient rises up onto tip toes Patient reports 21 93 .58 Hutchinson et al., 2013 49
Single heel and lowers back to the floor on pain on upward
raise the affected leg(s). or downward
movement
Patient places affected leg Patient reports pain 13 87 .43 Hutchinson et al., 2013 49
forward with toes forward at extreme range of
Passive
dorsiflexion and leans foot until can feel a motion
stretch on tendon. Patient heel
must not lift off ground.
Clinician palpates Achilles Clinician detects 3 100 .66 Hutchinson et al., 2013 49
tendon gently squeezing crepitation (could
between the index finger and detect “wet leather
Crepitus
thumb feeling for crepitation sign” signifying
with passive ankle movement. inflammation in
paratenon)
a Kappa can be interpreted as poor <.20, fair = .20 to .40, moderate = .40 to .60, good = .60 to .80, very good = .80 to 1.0. 148
b Three clinicians tested.
active with knee flexion since it crosses the knee joint while glyceryl trinitrate patches, (7) injection therapies (corticoste-
the soleus crosses only the ankle joint. If there is no difference roids, hyaluronic acid, platelet-rich plasma injections), (8)
in dorsiflexion with the knee flexed it is likely that there is shock wave therapy, and (9) low-level laser therapy. Patients
Achilles tendon and soleus muscle tightness. 57 who do not respond to conservative treatment may be candi-
dates for surgery, 47,60 but surgical treatments are not covered
here.
Conservative Treatment
In long-term follow-up studies, 80% to 84% of AT patients Nonsteroidal Anti-Inflammatory Drugs
returned to their normal activity with various conservative Nonsteroidal anti-inflammatory drugs (NSAIDs) have been
treatment plans, 58,59 although some tendon abnormalities may used extensively in AT to presumably reduce the pain associ-
58
60
persist. Studies on the effectiveness of several conservative ated with the disorder. NSAIDs inhibit cyclooxygenase en-
treatments for AT are discussed below and included only if zymes (COX1 and COX2), which are involved in the early
they specifically addressed AT. These treatments included the steps of prostaglandin formation. Inhibiting prostaglandins
61
use of (1) nonsteroidal anti-inflammatory medication, (2) ec- reduces inflammation and pain. In general, both oral and
centric exercise, (3) stretching, (4) orthotics, (5) bracing, (6) topical NSAIDs seem to provide short-term relief of pain for
Achilles Tendinopathy | 129