
Page 36 - Journal of Special Operations Medicine - Winter 2014
P. 36
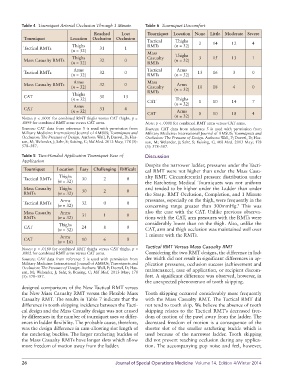
Table 4 Tourniquet Arterial Occlusion Through 1 Minute Table 6 Tourniquet Discomfort
Reached Lost Tourniquet Location None Little Moderate Severe
Tourniquet Location Occlusion Occlusion
Tactical Thighs
Thighs RMTs (n = 32) 2 14 12 4
Tactical RMTs 31 1
(n = 32)
Mass
Thighs Casualty Thighs 3 15 13 1
Mass Casualty RMTs 32 0 (n = 32)
(n = 32) RMTs
Arms Tactical Arms
Tactical RMTs 32 0 13 16 3 0
(n = 32) RMTs (n = 32)
Arms Mass
Mass Casualty RMTs 32 0 Arms
(n = 32) Casualty (n = 32) 10 18 4 0
RMTs
Thighs
CAT 30 13
(n = 32) Thighs
CAT 1 10 14 7
Arms (n = 32)
CAT 31 4
(n = 32) Arms
CAT 0 10 18 4
Notes: p < .0001 for combined RMT thighs versus CAT thighs. p = (n = 32)
.0099 for combined RMT arms versus CAT arms. Note: p < .0001 for combined RMT arms versus CAT arms.
Sources: CAT data from reference 5 is used with permission from Sources: CAT data from reference 5 is used with permission from
Military Medicine: International Journal of AMSUS; Tourniquets and Military Medicine: International Journal of AMSUS; Tourniquets and
Occlusion: The Pressure of Design. Authors: Wall, P; Duevel, D; Has- Occlusion: The Pressure of Design. Authors: Wall, P; Duevel, D; Has-
san, M; Welander, J; Sahr, S; Buising, C; Mil Med. 2013 May; 178 (5): san, M; Welander, J; Sahr, S; Buising, C; Mil Med. 2013 May; 178
578–587. (5): 578–587.
Table 5 Two-Handed Application Tourniquet Ease of Discussion
Application
Despite the narrower ladder, pressures under the Tacti-
Tourniquet Location Easy Challenging Difficult cal RMT were not higher than under the Mass Casu-
Thighs alty RMT. Circumferential pressure distribution under
Tactical RMTs 30 2 0
(n = 32) the Ratcheting Medical Tourniquets was not uniform
Mass Casualty Thighs 30 2 0 and tended to be higher under the Ladder than under
RMTs (n = 32) the Strap. RMT Occlusion, Completion, and 1 Minute
Arms pressures, especially on the thigh, were frequently in the
Tactical RMTs 32 0 0
(n = 32) concerning range greater than 300mmHg. This was
7
Mass Casualty Arms 31 1 0 also the case with the CAT. Unlike previous observa-
RMTs (n = 32) tions with the CAT, arm pressures with the RMTs were
Thighs considerably lower than on the thigh. Also, unlike the
CAT 24 8 0
(n = 32) CAT, arm and thigh occlusion was maintained well over
Arms 1 minute with the RMTs.
CAT 10 6 0
(n = 16)
Tactical RMT Versus Mass Casualty RMT
Notes: p = .0180 for combined RMT thighs versus CAT thighs. p =
.0002 for combined RMT arms versus CAT arms. Considering the two RMT designs, the difference in lad-
Sources: CAT data from reference 5 is used with permission from der width did not result in significant differences in ap-
Military Medicine: International Journal of AMSUS; Tourniquets and plication pressures, occlusion success (achievement and
Occlusion: The Pressure of Design. Authors: Wall, P; Duevel, D; Has- maintenance), ease of application, or recipient discom-
san, M; Welander, J; Sahr, S; Buising, C; Mil Med. 2013 May; 178
(5): 578–587. fort. A significant difference was observed, however, in
the unexpected phenomenon of tooth skipping.
designed comparisons of the New Tactical RMT versus
the New Mass Casualty RMT versus the Flexible Mass Tooth skipping occurred considerably more frequently
Casualty RMT. The results in Table 7 indicate that the with the Mass Casualty RMT. The Tactical RMT did
difference in tooth skipping incidence between the Tacti- not tend to tooth skip. We believe the absence of tooth
cal design and the Mass Casualty design was not caused skipping relates to the Tactical RMT’s decreased free-
by differences in the number of tourniquet uses or differ- dom of motion of the pawl away from the ladder. The
ences in ladder flexibility. The probable cause, therefore, decreased freedom of motion is a consequence of the
was the design difference in cam-allowing slot length of shorter slot of the smaller ratcheting buckle which is
the ratcheting buckles. The larger ratcheting buckles of used because of the narrower ladder. Tooth skipping
the Mass Casualty RMTs have longer slots which allow did not prevent reaching occlusion during any applica-
more freedom of motion away from the ladder. tion. The accompanying pop noise and feel, however,
26 Journal of Special Operations Medicine Volume 14, Edition 4/Winter 2014