
Page 32 - Journal of Special Operations Medicine - Winter 2014
P. 32
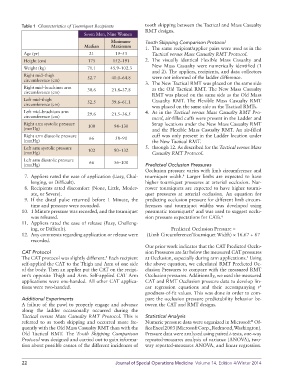
Table 1 Characteristics of Tourniquet Recipients tooth skipping between the Tactical and Mass Casualty
RMT designs.
Seven Men, Nine Women
Minimum- Tooth Skipping Comparison Protocol
Median Maximum 1. The same recipient/applier pairs were used as in the
Age (yr) 21 19–53 Tactical versus Mass Casualty RMT Protocol.
Height (cm) 175 152–191 2. The visually identical Flexible Mass Casualty and
New Mass Casualty were numerically identified (1
Weight (kg) 71.1 45.9–102.3
and 2). The appliers, recipients, and data collectors
Right mid–thigh 52.7 40.0–64.8 were not informed of the ladder difference.
circumference (cm)
3. The New Tactical RMT was placed on the same side
Right mid–brachium arm 30.6 21.8–37.8 as the Old Tactical RMT. The New Mass Casualty
circumference (cm)
RMT was placed on the same side as the Old Mass
Left mid–thigh 52.5 39.6–61.1 Casualty RMT. The Flexible Mass Casualty RMT
circumference (cm) was placed on the same side as the Tactical RMTs.
Left mid–brachium arm 29.6 21.5–36.5 4. As in the Tactical versus Mass Casualty RMT Pro-
circumference (cm) tocol, air-filled cuffs were present in the Ladder and
Right arm systolic pressure 100 94–130 Strap locations under the New Mass Casualty RMT
(mmHg) and the Flexible Mass Casualty RMT. An air-filled
Right arm diastolic pressure 66 58–90 cuff was only present in the Ladder location under
(mmHg) the New Tactical RMT.
Left arm systolic pressure 102 90–132 5. through 12. As described for the Tactical versus Mass
(mmHg) Casualty RMT Protocol.
Left arm diastolic pressure 66 56–100
(mmHg) Predicted Occlusion Pressures
Occlusion pressure varies with limb circumference and
7. Appliers rated the ease of application (Easy, Chal- tourniquet width. Larger limbs are expected to have
4
lenging, or Difficult). higher tourniquet pressures at arterial occlusion. Nar-
8. Recipients rated discomfort (None, Little, Moder- rower tourniquets are expected to have higher tourni-
ate, or Severe). quet pressures at arterial occlusion. An equation for
9. If the distal pulse returned before 1 Minute, the predicting occlusion pressure for different limb circum-
time and pressure were recorded. ferences and tourniquet widths was developed using
10. 1 Minute pressure was recorded, and the tourniquet pneumatic tourniquets and was used to suggest occlu-
4
was released. sion pressure expectations for CATs. 6
11. Appliers rated the ease of release (Easy, Challeng-
ing, or Difficult). Predicted Occlusion Pressure =
12. Any comments regarding application or release were (Limb Circumference/Tourniquet Width) × 16.67 + 67
recorded.
Our prior work indicates that the CAT Predicted Occlu-
CAT Protocol sion Pressures are far below the measured CAT pressures
The CAT protocol was slightly different. Each recipient at Occlusion, especially during arm applications. Using
5
5
self-applied the CAT to the Thigh and Arm of one side the above equation, we calculated RMT Predicted Oc-
of the body. Then an applier put the CAT on the recipi- clusion Pressures to compare with the measured RMT
ent’s opposite Thigh and Arm. Self-applied CAT Arm Occlusion pressures. Additionally, we used the measured
applications were one-handed. All other CAT applica- CAT and RMT Occlusion pressure data to develop lin-
tions were two-handed. ear regression equations and their accompanying r
2
goodness-of-fit values. This was done in order to com-
Additional Experiments pare the occlusion pressure predictability behavior be-
A failure of the pawl to properly engage and advance tween the CAT and RMT designs.
along the ladder occasionally occurred during the
Tactical versus Mass Casualty RMT Protocol. This is Statistical Analysis
referred to as tooth skipping and occurred more fre- Numeric pressure data were organized in Microsoft Of-
®
quently with the Old Mass Casualty RMT than with the fice Excel 2003 (Microsoft Corp., Redmond, Washington).
Old Tactical RMT. The Tooth Skipping Comparison Pressure data were analyzed using paired t-tests, one-way
Protocol was designed and carried out to gain informa- repeated-measures analysis of variance (ANOVA), two-
tion about possible causes of the different incidences of way repeated-measures ANOVA, and linear regression.
22 Journal of Special Operations Medicine Volume 14, Edition 4/Winter 2014