
Page 75 - ATP-P 11th Ed
P. 75
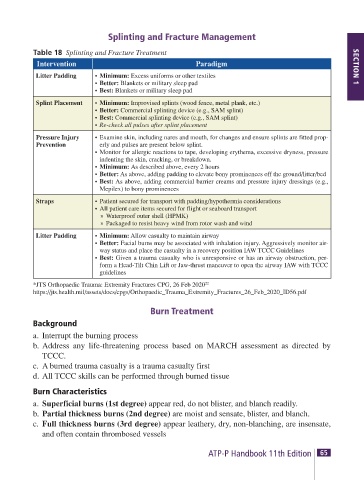
Splinting and Fracture Management
Table 18 Splinting and Fracture Treatment
Intervention Paradigm SECTION 1
Litter Padding • Minimum: Excess uniforms or other textiles
• Better: Blankets or military sleep pad
• Best: Blankets or military sleep pad
Splint Placement • Minimum: Improvised splints (wood fence, metal plank, etc.)
• Better: Commercial splinting device (e.g., SAM splint)
• Best: Commercial splinting device (e.g., SAM splint)
• Re-check all pulses after splint placement
Pressure Injury • Examine skin, including nares and mouth, for changes and ensure splints are fitted prop-
Prevention erly and pulses are present below splint.
• Monitor for allergic reactions to tape, developing erythema, excessive dryness, pressure
indenting the skin, cracking, or breakdown.
• Minimum: As described above, every 2 hours
• Better: As above, adding padding to elevate bony prominences off the ground/litter/bed
• Best: As above, adding commercial barrier creams and pressure injury dressings (e.g.,
Mepilex) to bony prominences
Straps • Patient secured for transport with padding/hypothermia considerations
• All patient care items secured for flight or seaboard transport
» Waterproof outer shell (HPMK)
» Packaged to resist heavy wind from rotor wash and wind
Litter Padding • Minimum: Allow casualty to maintain airway
• Better: Facial burns may be associated with inhalation injury. Aggressively monitor air-
way status and place the casualty in a recovery position IAW TCCC Guidelines
• Best: Given a trauma casualty who is unresponsive or has an airway obstruction, per-
form a Head-Tilt Chin Lift or Jaw-thrust maneuver to open the airway IAW with TCCC
guidelines
*JTS Orthopaedic Trauma: Extremity Fractures CPG, 26 Feb 2020 22
https://jts.health.mil/assets/docs/cpgs/Orthopaedic_Trauma_Extremity_Fractures_26_Feb_2020_ID56.pdf
Burn Treatment
Background
a. Interrupt the burning process
b. Address any life-threatening process based on MARCH assessment as directed by
TCCC.
c. A burned trauma casualty is a trauma casualty first
d. All TCCC skills can be performed through burned tissue
Burn Characteristics
a. Superficial burns (1st degree) appear red, do not blister, and blanch readily.
b. Partial thickness burns (2nd degree) are moist and sensate, blister, and blanch.
c. Full thickness burns (3rd degree) appear leathery, dry, non-blanching, are insensate,
and often contain thrombosed vessels
64 SECTION 1 TACTICAL TRAUMA PROTOCOLS (TTPs) ATP-P Handbook 11th Edition 65