
Page 72 - ATP-P 11th Ed
P. 72
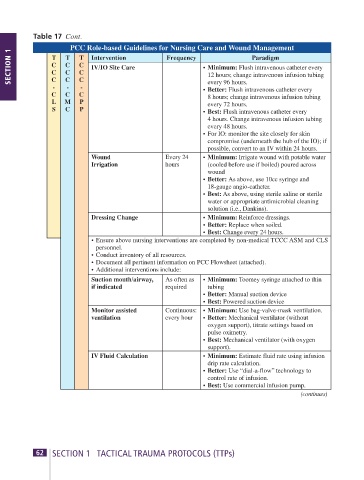
Table 17 Cont.
PCC Role-based Guidelines for Nursing Care and Wound Management
SECTION 1 T T T Intervention Frequency • Minimum: Flush intravenous catheter every
Paradigm
C C
C
IV/IO Site Care
C
C C
12 hours; change intravenous infusion tubing
C
every 96 hours.
- C - C - • Better: Flush intravenous catheter every
C C C 8 hours; change intravenous infusion tubing
L M P every 72 hours.
S C P • Best: Flush intravenous catheter every
4 hours. Change intravenous infusion tubing
every 48 hours.
• For IO: monitor the site closely for skin
compromise (underneath the hub of the IO); if
possible, convert to an IV within 24 hours.
Wound Every 24 • Minimum: Irrigate wound with potable water
Irrigation hours (cooled before use if boiled) poured across
wound
• Better: As above, use 10cc syringe and
18-gauge angio-catheter.
• Best: As above, using sterile saline or sterile
water or appropriate antimicrobial cleaning
solution (i.e., Dankins).
Dressing Change • Minimum: Reinforce dressings.
• Better: Replace when soiled.
• Best: Change every 24 hours.
• Ensure above nursing interventions are completed by non-medical TCCC ASM and CLS
personnel.
• Conduct inventory of all resources.
• Document all pertinent information on PCC Flowsheet (attached).
• Additional interventions include:
Suction mouth/airway, As often as • Minimum: Toomey syringe attached to thin
if indicated required tubing
• Better: Manual suction device
• Best: Powered suction device
Monitor assisted Continuous: • Minimum: Use bag-valve-mask ventilation.
ventilation every hour • Better: Mechanical ventilator (without
oxygen support), titrate settings based on
pulse oximetry.
• Best: Mechanical ventilator (with oxygen
support).
IV Fluid Calculation • Minimum: Estimate fluid rate using infusion
drip rate calculation.
• Better: Use “dial-a-flow” technology to
control rate of infusion.
• Best: Use commercial infusion pump.
(continues)
62 SECTION 1 TACTICAL TRAUMA PROTOCOLS (TTPs) ATP-P Handbook 11th Edition 63