
Page 16 - JSOM Spring 2025
P. 16
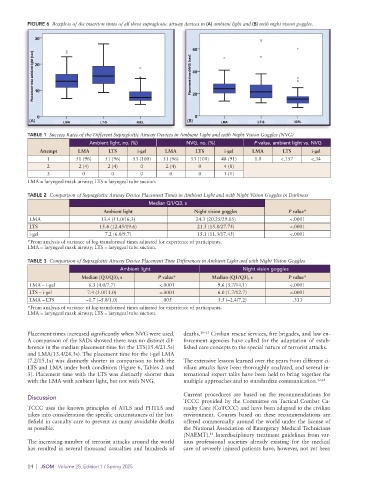
FIGURE 6 Boxplots of the insertion times of all three supraglottic airway devices in (A) ambient light and (B) with night vision goggles.
(A) (B)
TABLE 1 Success Rates of the Different Supraglottic Airway Devices in Ambient Light and with Night Vision Goggles (NVG)
Ambient light, no. (%) NVG, no. (%) P value, ambient light vs. NVG
Attempt LMA LTS i-gel LMA LTS i-gel LMA LTS i-gel
1 51 (96) 51 (96) 53 (100) 51 (96) 53 (100) 48 (91) 1.0 <.157 <.34
2 2 (4) 2 (4) 0 2 (4) 0 4 (8)
3 0 0 0 0 0 1 (1)
LMA = laryngeal mask airway; LTS = laryngeal tube suction.
TABLE 2 Comparison of Supraglottic Airway Device Placement Times in Ambient Light and with Night Vision Goggles in Darkness
Median Q1/Q3, s
Ambient light Night vision goggles P value*
LMA 13.4 (11.0/16.3) 24.3 (20.25/29.05) <.0001
LTS 15.4 (12.45/19.6) 21.5 (15.8/27.75) <.0001
i-gel 7.2 (6.0/9.7) 15.1 (11.3/17.45) <.0001
*From analysis of variance of log-transformed times adjusted for experience of participants.
LMA = laryngeal mask airway; LTS = laryngeal tube suction.
TABLE 3 Comparison of Supraglottic Airway Device Placement Time Differences in Ambient Light and with Night Vision Goggles
Ambient light Night vision goggles
Median (Q1/Q3), s P value* Median (Q1/Q3), s P value*
LMA – i-gel 6.3 (4.0/7.7) <.0001 9.6 (3.7/14.1) <.0001
LTS – i-gel 7.4 (5.0/11.0) <.0001 6.0 (1.7/12.7) <.0001
LMA – LTS –1.7 (–5.8/1.0) .005 3.5 (–2.4/7.2) .313
*From analysis of variance of log-transformed times adjusted for experience of participants.
LMA = laryngeal mask airway; LTS = laryngeal tube suction.
Placement times increased significantly when NVG were used. deaths. 10–12 Civilian rescue services, fire brigades, and law en-
A comparison of the SADs showed there was no distinct dif- forcement agencies have called for the adaptation of estab-
ference in the median placement time for the LTS(15.4/21.5s) lished care concepts to the special nature of terrorist attacks.
and LMA(13.4/24.3s). The placement time for the i-gel LMA
(7.2/15.1s) was distinctly shorter in comparison to both the The extensive lessons learned over the years from different ci-
LTS and LMA under both conditions (Figure 6, Tables 2 and vilian attacks have been thoroughly analyzed, and several in-
3). Placement time with the LTS was distinctly shorter than ternational expert talks have been held to bring together the
with the LMA with ambient light, but not with NVG. multiple approaches and to standardize communication. 13,14
Current procedures are based on the recommendations for
Discussion
TCCC provided by the Committee on Tactical Combat Ca-
TCCC uses the known principles of ATLS and PHTLS and sualty Care (CoTCCC) and have been adapted to the civilian
takes into consideration the specific circumstances of the bat- environment. Courses based on these recommendations are
tlefield in casualty care to prevent as many avoidable deaths offered commercially around the world under the license of
as possible. the National Association of Emergency Medical Technicians
(NAEMT). Interdisciplinary treatment guidelines from var-
15
The increasing number of terrorist attacks around the world ious professional societies already existing for the medical
has resulted in several thousand casualties and hundreds of care of severely injured patients have, however, not yet been
14 | JSOM Volume 25, Edition 1 / Spring 2025