
Page 29 - JSOM Spring 2023
P. 29
SUPPLEMENTAL TABLE 2 Volumes of Procedures by Year
Year Intubations Intubation Death % Cricothyrotomy Cricothyrotomy Death % SGA SGA Death %
2007 176 36.9 26 42.3 1 100
2008 134 14.1 17 47.0 0 0
2009 82 24.3 23 47.8 0 0
2010 242 19.4 47 36.1 1 100
2011 219 20.0 38 55.2 3 33.3
2012 138 18.8 29 41.3 10 50
2013 82 30.4 22 36.3 12 50
2014 42 30.9 7 57.1 0 0
2015 9 33.3 5 20 2 0
2016 10 0 3 33.3 0 0
2017 2 0 10 10 1 100
2018 2 0 9 11.1 2 0
2019 9 22.2 15 20 3 33.3
SGA = supraglottic airway
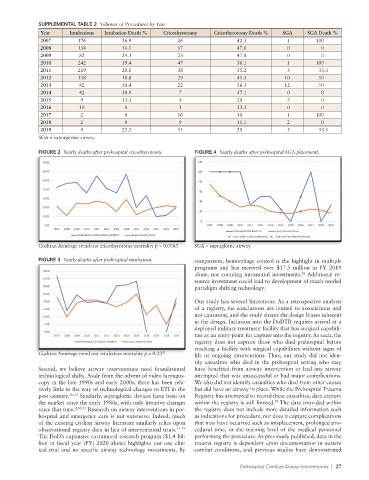
FIGURE 2 Yearly deaths after prehospital cricothyrotomy. FIGURE 4 Yearly deaths after prehospital SGA placement.
Cochran Armitage trend test cricothyrotomy mortality p = 0.0063 SGA = supraglottic airway
FIGURE 3 Yearly deaths after prehospital intubation. comparison, hemorrhage control is the highlight in multiple
programs and has received over $17.5 million in FY 2019
alone, not counting intramural investments. Additional re-
38
source investment could lead to development of much needed
paradigm shifting technology.
Our study has several limitations. As a retrospective analysis
of a registry, the conclusions are limited to associations and
not causation, and the study shares the design biases inherent
in the design. Inclusion into the DoDTR requires arrival at a
deployed military treatment facility that has surgical capabili-
ties as an entry point for capture into the registry. As such, the
registry does not capture those who died prehospital before
reaching a facility with surgical capabilities without signs of
Cochran Armitage trend test intubation mortality p = 0.237 life or ongoing interventions. Thus, our study did not iden-
tify casualties who died in the prehospital setting who may
Second, we believe airway interventions need foundational have benefited from airway intervention or had any airway
technological shifts. Aside from the advent of video laryngos- attempted that was unsuccessful or had major complications.
copy in the late 1990s and early 2000s, there has been rela- We also did not identify casualties who died from other causes
tively little in the way of technological changes to ETI in the but did have an airway in place. While the Prehospital Trauma
past century. 30–33 Similarly, supraglottic devices have been on Registry has attempted to record these casualties, data capture
the market since the early 1980s, with only iterative changes within the registry is still limited. The data provided within
39
since that time. 4,30,34 Research on airway interventions in pre- the registry does not include more detailed information such
hospital and emergency care is not extensive. Indeed, much as indications for procedure, nor does it capture complications
of the existing civilian airway literature similarly relies upon that may have occurred such as misplacement, prolonged pro-
observational registry data in lieu of interventional trials. 35–37 cedural time, or the training level of the medical personnel
The DoD’s expansive extramural research program ($1.4 bil- performing the procedure. As previously published, data in the
lion in fiscal year (FY) 2020 alone) highlights just one clin- trauma registry is dependent upon documentation in austere
ical trial and no specific airway technology investments. By combat conditions, and previous studies have demonstrated
Prehospital Combat Airway Interventions | 27