
Page 22 - JSOM Winter 2022
P. 22
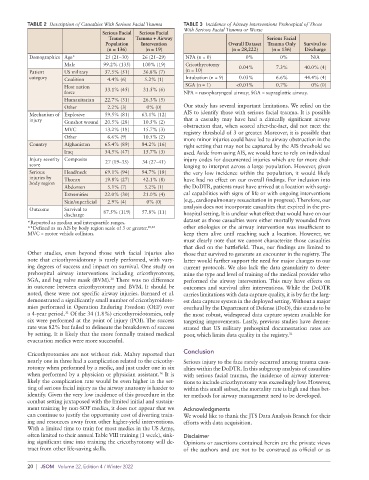
TABLE 2 Description of Casualties With Serious Facial Trauma TABLE 3 Incidence of Airway Interventions Prehospital of Those
With Serious Facial Trauma or Worse
Serious Facial Serious Facial
Trauma Trauma + Airway Serious Facial
Population Intervention Overall Dataset Trauma Only Survival to
(n = 136) (n = 19) (n = 28,222) (n = 136) Discharge
Demographics Age* 25 (21–30) 26 (21–29) NPA (n = 0) 0% 0% N/A
Male 99.2% (135) 100% (19) Cricothyrotomy 0.04% 7.3% 40.0% (4)
Patient US military 37.5% (51) 36.8% (7) (n = 10)
category Coalition 4.4% (6) 5.2% (1) Intubation (n = 9) 0.03% 6.6% 44.4% (4)
Host nation 33.1% (45) 31.5% (6) SGA (n = 1) <0.01% 0.7% 0% (0)
force NPA = nasopharyngeal airway; SGA = supraglottic airway.
Humanitarian 22.7% (31) 26.3% (5)
Other 2.2% (3) 0% (0) Our study has several important limitations. We relied on the
Mechanism of Explosive 59.5% (81) 63.1% (12) AIS to identify those with serious facial trauma. It is possible
injury Gunshot wound 20.5% (28) 10.5% (2) that a casualty may have had a clinically significant airway
MVC 13.2% (18) 15.7% (3) obstruction that, when scored after-the-fact, did not meet the
registry threshold of 3 or greater. Moreover, it is possible that
Other 6.6% (9) 10.5% (2) more minor injuries could have led to airway obstruction in the
Country Afghanistan 65.4% (89) 84.2% (16) right setting that may not be captured by the AIS threshold we
Iraq 34.5% (47) 15.7% (3) used. Aside from using AIS, we would have to rely on individual
Injury severity Composite 27 (19–35) 34 (27–41) injury codes for documented injuries which are far more chal-
score lenging to interpret across a large population. However, given
Serious Head/neck 69.1% (94) 94.7% (18) the very low incidence within the population, it would likely
injuries by Thorax 19.8% (27) 42.1% (8) have had no effect on our overall findings. For inclusion into
body region
Abdomen 5.1% (7) 5.2% (1) the DoDTR, patients must have arrived at a location with surgi-
Extremities 22.0% (30) 21.0% (4) cal capabilities with signs of life or with ongoing interventions
Skin/superficial 2.9% (4) 0% (0) (e.g., cardiopulmonary resuscitation in progress). Therefore, our
Outcome Survival to analysis does not incorporate casualties that expired in the pre-
discharge 87.5% (119) 57.8% (11) hospital setting. It is unclear what effect that would have on our
*Reported as median and interquartile ranges. dataset as those casualties were either mortally wounded from
**Defined as an AIS by body region scale of 3 or greater. 20,28 other etiologies or the airway intervention was insufficient to
MVC = motor vehicle collision. keep them alive until reaching such a location. However, we
must clearly note that we cannot characterize those casualties
that died on the battlefield. Thus, our findings are limited to
Other studies, even beyond those with facial injuries also those that survived to generate an encounter in the registry. The
note that cricothyroidotomy is rarely performed, with vary- latter would further support the need for major changes to our
ing degrees of success and impact on survival. One study on current protocols. We also lack the data granularity to deter-
prehospital airway interventions including cricothyrotomy, mine the type and level of training of the medical provider who
SGA, and bag valve mask (BVM). There was no difference performed the airway intervention. This may have effects on
30
in outcome between cricothyrotomy and BVM. It should be outcomes and survival after interventions. While the DoDTR
noted, these were not specific airway injuries. Barnard et al. carries limitations with data capture quality, it is by far the larg-
demonstrated a significantly small number of cricothyroidoto- est data capture system in the deployed setting. Without a major
mies performed in Operation Enduring Freedom (OEF) over overhaul by the Department of Defense (DoD), this stands to be
a 4-year period. Of the 34 (1.8%) cricothyroidotomies, only the most robust, widespread data capture system available for
31
six were performed at the point of injury (POI). The success targeting improvements. Lastly, previous studies have demon-
rate was 82% but failed to delineate the breakdown of success strated that US military prehospital documentation rates are
by setting. It is likely that the more formally trained medical poor, which limits data quality in the registry. 32
evacuation medics were more successful.
Cricothyrotomies are not without risk. Mabry reported that Conclusion
nearly one in three had a complication related to the cricothy- Serious injury to the face rarely occurred among trauma casu-
rotomy when performed by a medic, and just under one in six alties within the DoDTR. In this subgroup analysis of casualties
when performed by a physician or physician assistant. It is with serious facial trauma, the incidence of airway interven-
16
likely the complication rate would be even higher in the set- tions to include cricothyrotomy was exceedingly low. However,
ting of serious facial injury as the airway anatomy is harder to within this small subset, the mortality rate is high and thus bet-
identify. Given the very low incidence of this procedure in the ter methods for airway management need to be developed.
combat setting juxtaposed with the limited initial and sustain-
ment training by non-SOF medics, it does not appear that we Acknowledgments
can continue to justify the opportunity cost of diverting train- We would like to thank the JTS Data Analysis Branch for their
ing and resources away from other higher-yield interventions. efforts with data acquisition.
With a limited time to train for most medics in the US Army,
often limited to their annual Table VIII training (1 week), sink- Disclaimer
ing significant time into training the cricothyrotomy will de- Opinions or assertions contained herein are the private views
tract from other life-saving skills. of the authors and are not to be construed as official or as
20 | JSOM Volume 22, Edition 4 / Winter 2022