
Page 115 - JSOM Summer 2022
P. 115
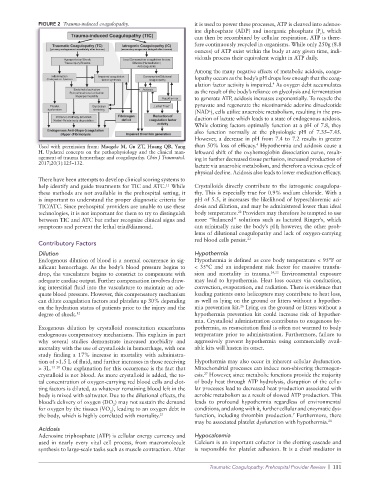
FIGURE 2 Trauma-induced coagulopathy. it is used to power these processes, ATP is cleaved into adenos-
ine diphosphate (ADP) and inorganic phosphate (P ), which
i
can then be recombined by cellular respiration. ATP is there-
fore continuously recycled in organisms. While only 250g (8.8
ounces) of ATP exist within the body at any given time, indi-
viduals process their equivalent weight in ATP daily.
Among the many negative effects of metabolic acidosis, coagu-
lopathy occurs as the body’s pH drops low enough that the coag-
ulation factor activity is impaired. As oxygen debt accumulates
4
as the result of the body’s reliance on glycolysis and fermentation
to generate ATP, acidosis increases exponentially. To recycle the
pyruvate and regenerate the nicotinamide adenine dinucleotide
(NAD ), cells utilize anaerobic metabolism, resulting in the pro-
+
duction of lactate which leads to a state of endogenous acidosis.
While clotting factors optimally function at a pH of 7.8, they
also function normally at the physiologic pH of 7.35–7.45.
However, a decrease in pH from 7.4 to 7.2 results in greater
4
Used with permission from: Maegele M, Gu ZT, Huang QB, Yang than 50% loss of efficacy. Hypothermia and acidosis cause a
H. Updated concepts on the pathophysiology and the clinical man- leftward shift of the oxyhemoglobin dissociation curve, result-
agement of trauma hemorrhage and coagulopathy. Chin J Traumatol. ing in further decreased tissue perfusion, increased production of
2017;20(3):125–132. lactate via anaerobic metabolism, and therefore a vicious cycle of
physical decline. Acidosis also leads to lower medication efficacy.
There have been attempts to develop clinical scoring systems to
help identify and guide treatments for TIC and ATC. While Crystalloids directly contribute to the iatrogenic coagulopa-
11
these methods are not available in the prehospital setting, it thy. This is especially true for 0.9% sodium chloride. With a
is important to understand the proper diagnostic criteria for pH of 5.5, it increases the likelihood of hyperchloremic aci-
TIC/ATC. Since prehospital providers are unable to use these dosis and dilution, and may be administered lower than ideal
22
technologies, it is not important for them to try to distinguish body temperature. Providers may therefore be tempted to use
between TIC and ATC but rather recognize clinical signs and more “balanced” solutions such as lactated Ringer’s, which
symptoms and prevent the lethal triad/diamond. can minimally raise the body’s pH; however, the other prob-
lems of dilutional coagulopathy and lack of oxygen-carrying
red blood cells persist. 23
Contributory Factors
Dilution Hypothermia
Endogenous dilution of blood is a normal occurrence in sig- Hypothermia is defined as core body temperature < 95°F or
nificant hemorrhage. As the body’s blood pressure begins to < 35°C and an independent risk factor for massive transfu-
drop, the vasculature begins to constrict to compensate with sion and mortality in trauma. 24,25 Environmental exposure
adequate cardiac output. Further compensation involves draw- may lead to hypothermia. Heat loss occurs via conduction,
ing interstitial fluid into the vasculature to maintain an ade- convection, evaporation, and radiation. There is evidence that
quate blood pressure. However, this compensatory mechanism loading patients onto helicopters may contribute to heat loss,
can dilute coagulation factors and platelets up 30% depending as well as lying on the ground or litters without a hypother-
on the hydration status of patients prior to the injury and the mia prevention kit. Lying on the ground or litters without a
26
degree of shock. 12 hypothermia prevention kit could increase risk of hypother-
mia. Crystalloid administration contributes to exogenous hy-
Exogenous dilution by crystalloid resuscitation exacerbates pothermia, as resuscitation fluid is often not warmed to body
endogenous compensatory mechanisms. This explains in part temperature prior to administration. Furthermore, failure to
why several studies demonstrate increased morbidity and aggressively prevent hypothermia using commercially avail-
mortality with the use of crystalloids in hemorrhage, with one able kits will hasten its onset.
study finding a 17% increase in mortality with administra-
tion of >1.5 L of fluid, and further increases in those receiving Hypothermia may also occur in inherent cellular dysfunction.
> 3L. 13–20 One explanation for this occurrence is the fact that Mitochondrial processes can induce non-shivering thermogen-
crystalloid is not blood. As more crystalloid is added, the to- esis. However, since metabolic functions provide the majority
27
tal concentration of oxygen-carrying red blood cells and clot- of body heat through ATP hydrolysis, disruption of the cellu-
ting factors is diluted, as whatever remaining blood left in the lar processes lead to decreased heat production associated with
body is mixed with saltwater. Due to the dilutional effects, the aerobic metabolism as a result of slowed ATP production. This
blood’s delivery of oxygen (DO ) may not sustain the demand leads to profound hypothermia regardless of environmental
2
for oxygen by the tissues (VO ), leading to an oxygen debt in conditions, and along with it, further cellular and enzymatic dys-
2
7
the body, which is highly correlated with mortality. 21 function, including thrombin production. Furthermore, there
may be associated platelet dysfunction with hypothermia. 28
Acidosis
Adenosine triphosphate (ATP) is cellular energy currency and Hypocalcemia
used in nearly every vital cell process, from macromolecule Calcium is an important cofactor in the clotting cascade and
synthesis to large-scale tasks such as muscle contraction. After is responsible for platelet adhesion. It is a chief mediator in
Traumatic Coagulopathy: Prehospital Provider Review | 111