
Page 32 - 2022 Spring JSOM
P. 32
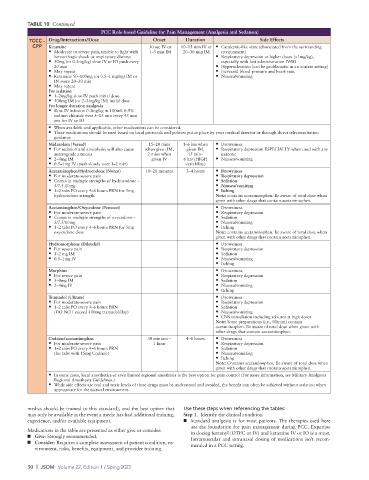
TABLE 10 Continued
PCC Role-based Guideline for Pain Management (Analgesia and Sedation)
TCCC - Drug/Interactions/Dose Onset Duration Side Effects
CPP Ketamine 30 sec IV or 10–15 min IV or • Cataleptic-like state (dissociated from the surrounding
• Moderate to severe pain, unable to fight with 1–5 min IM 20–30 min IM environment)
hemorrhagic shock or respiratory distress • Respiratory depression at higher doses (>1mg/kg),
• 30mg (or 0.3mg/kg) slow IV or IO push every especially with fast administration IV/IO
20 min • Hypersalivation (can be problematic in an austere setting)
• May repeat • Increased blood pressure and heart rate.
• Ketamine 50–100mg (or 0.5–1 mg/kg) IM or • Nausea/vomiting
IN every 20–30 min
• May repeat
For sedation
• 1–2mg/kg slow IV push initial dose
• 300mg IM (or 2–3mg/kg IM) initial dose
For longer duration analgesia
• Slow IV infusion 0.3mg/kg in 100mL 0.9%
sodium chloride over 5–15 min every 45 min
prn for IV or IO
• When available and applicable, other medications can be considered.
• These medications should be used based on local protocols and policies put in place by your medical director or through direct teleconsultation
guidance.
Midazolam (Versed) 15–20 mins 1–6 hrs when • Drowsiness
• For sedation and anxiolysis; will also cause when given IM, given IM, • Respiratory depression ESPECIALLY when used with any
anterograde amnesia 2 mins when 15 min– narcotic
• 2–4mg IM given IV 6 hrs (HIGH • Nausea/vomiting
• 0.5–1mg IV (push slowly over 1–2 min) variability)
Acetaminophen/Hydrocodone (Norco) 10–20 minutes 3–4 hours • Drowsiness
• For moderate-severe pain • Respiratory depression
• Comes in multiple strengths of hydrocodone – • Sedation
5/7.5.10mg • Nausea/vomiting
• 1–2 tabs PO every 4–6 hours PRN for 5mg • Itching
hydrocodone strength Note: contains acetaminophen. Be aware of total dose when
given with other drugs that contain acetaminophen.
Acetaminophen/Oxycodone (Percocet) • Drowsiness
• For moderate-severe pain • Respiratory depression
• Comes in multiple strengths of oxycodone – • Sedation
5/7.5/10mg • Nausea/vomiting
• 1–2 tabs PO every 4–6 hours PRN for 5mg • Itching
oxycodone dose Note: contains acetaminophen. Be aware of total dose when
given with other drugs that contain acetaminophen.
Hydromorphone (Dilaudid) • Drowsiness
• For severe pain • Respiratory depression
• 1–2 mg IM • Sedation
• 0.5–1mg IV • Nausea/vomiting
• Itching
Morphine • Drowsiness
• For severe pain • Respiratory depression
• 5–0mg IM • Sedation
• 2–4mg IV • Nausea/vomiting
• Itching
Tramadol (Ultram) • Drowsiness
• For moderate-severe pain • Respiratory depression
• 1–2 tabs PO every 4–6 hours PRN • Sedation
(DO NOT exceed 400mg tramadol/day) • Nausea/vomiting
• CNS stimulation including seizures at high doses
Note: Some preparations (i.e., Ultram) contain
acetaminophen. Be aware of total dose when given with
other drugs that contain acetaminophen.
Codeine/acetaminophen 30 minutes – 4–6 hours • Drowsiness
• For moderate-severe pain 1 hour • Respiratory depression
• 1–2 tabs PO every 4–6 hours PRN • Sedation
(for tabs with 15mg Codeine) • Nausea/vomiting
• Itching
Note: Contains acetaminophen. Be aware of total dose when
given with other drugs that contain acetaminophen.
• In some cases, local anesthetics or even limited regional anesthesia is the best option for pain control (For more information, see Military Analgesia
Regional Anesthesia Guidelines.)
• While side effects are real and toxic levels of these drugs must be understood and avoided, the benefit can often be achieved without sedation when
appropriate for the tactical environment.
medics should be trained to this standard), and the best option that Use these steps when referencing the tables:
may only be available in the event a medic has had additional training, Step 1. Identify the clinical condition
experience, and/or available equipment. ■ Standard analgesia is for most patients. The therapies used here
are the foundation for pain management during PCC. Expertise
Medications in the table are presented as either give or consider: in dosing fentanyl (OTFC or IV) and ketamine IV or IO is a must.
■ Give: Strongly recommended. Intramuscular and intranasal dosing of medications isn’t recom-
■ Consider: Requires a complete assessment of patient condition, en- mended in a PCC setting.
vironment, risks, benefits, equipment, and provider training.
30 | JSOM Volume 22, Edition 1 / Sping 2022