
Page 15 - JSOM Fall 2021
P. 15
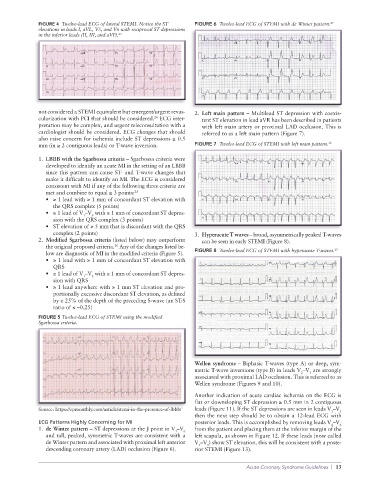
FIGURE 4 Twelve-lead ECG of lateral STEMI. Notice the ST FIGURE 6 Twelve-lead ECG of STEMI with de Winter pattern. 27
elevations in leads I, aVL, V5, and V6 with reciprocal ST depressions
in the inferior leads (II, III, and aVF). 23
not considered a STEMI equivalent but emergent/urgent revas- 2. Left main pattern – Multilead ST depression with coexis-
24
cularization with PCI that should be considered. ECG inter- tent ST elevation in lead aVR has been described in patients
pretation may be complex, and urgent teleconsultation with a with left main artery or proximal LAD occlusion. This is
cardiologist should be considered. ECG changes that should referred to as a left main pattern (Figure 7).
also raise concern for ischemia include ST depressions ≥ 0.5
mm (in ≥ 2 contiguous leads) or T-wave inversion. FIGURE 7 Twelve-lead ECG of STEMI with left main pattern. 28
1. LBBB with the Sgarbossa criteria – Sgarbossa criteria were
developed to identify an acute MI in the setting of an LBBB
since this pattern can cause ST- and T-wave changes that
make it difficult to identify an MI. The ECG is considered
consistent with MI if any of the following three criteria are
met and combine to equal ≥ 3 points: 25
• ≥ 1 lead with ≥ 1 mm of concordant ST elevation with
the QRS complex (5 points)
• ≥ 1 lead of V –V with ≥ 1 mm of concordant ST depres-
3
1
sion with the QRS complex (3 points)
• ST elevation of ≥ 5 mm that is discordant with the QRS
complex (2 points) 3. Hyperacute T waves – broad, asymmetrically peaked T-waves
2. Modified Sgarbossa criteria (listed below) may outperform can be seen in early STEMI (Figure 8).
26
the original proposed criteria. Any of the changes listed be- 29
low are diagnostic of MI in the modified criteria (Figure 5). FIGURE 8 Twelve-lead ECG of STEMI with hyperacute T-waves.
• ≥ 1 lead with ≥ 1 mm of concordant ST elevation with
QRS
• ≥ 1 lead of V –V with ≥ 1 mm of concordant ST depres-
1
3
sion with QRS
• ≥ 1 lead anywhere with ≥ 1 mm ST elevation and pro-
portionally excessive discordant ST elevation, as defined
by ≥ 25% of the depth of the preceding S-wave (an ST:S
ratio of ≤ –0.25)
FIGURE 5 Twelve-lead ECG of STEMI using the modified
Sgarbossa criteria.
Wellen syndrome – Biphasic T-waves (type A) or deep, sym-
metric T-wave inversions (type B) in leads V –V are strongly
3
2
associated with proximal LAD occlusion. This is referred to as
Wellen syndrome (Figures 9 and 10).
Another indication of acute cardiac ischemia on the ECG is
flat or downsloping ST depression ≥ 0.5 mm in 2 contiguous
Source: https://epmonthly.com/article/stemi-in-the-presence-of-lbbb/ leads (Figure 11). If the ST depressions are seen in leads V –V
1
3
then the next step should be to obtain a 12-lead ECG with
ECG Patterns Highly Concerning for MI posterior leads. This is accomplished by removing leads V –V
4
6
1. de Winter pattern – ST depressions at the J point in V –V from the patient and placing them at the inferior margin of the
1
6
and tall, peaked, symmetric T-waves are consistent with a left scapula, as shown in Figure 12. If these leads (now called
de Winter pattern and associated with proximal left anterior V –V ) show ST elevation, this will be consistent with a poste-
7
9
descending coronary artery (LAD) occlusion (Figure 6). rior STEMI (Figure 13).
Acute Coronary Syndrome Guidelines | 13