
Page 16 - JSOM Fall 2021
P. 16
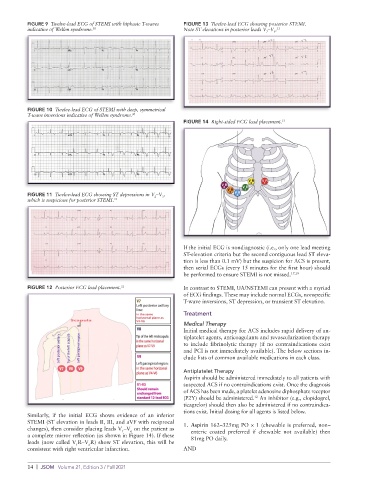
FIGURE 9 Twelve-lead ECG of STEMI with biphasic T-waves FIGURE 13 Twelve-lead ECG showing posterior STEMI.
indicative of Wellen syndrome. 30 Note ST elevations in posterior leads V –V . 9 31
7
FIGURE 10 Twelve-lead ECG of STEMI with deep, symmetrical
T-wave inversions indicative of Wellen syndrome. 30
FIGURE 14 Right-sided ECG lead placement. 33
FIGURE 11 Twelve-lead ECG showing ST depressions in V –V ,
3
2
which is suspicious for posterior STEMI. 31
If the initial ECG is nondiagnostic (i.e., only one lead meeting
ST-elevation criteria but the second contiguous lead ST eleva-
tion is less than 0.1 mV) but the suspicion for ACS is present,
then serial ECGs (every 15 minutes for the first hour) should
be performed to ensure STEMI is not missed. 17,19
FIGURE 12 Posterior ECG lead placement. 32 In contrast to STEMI, UA/NSTEMI can present with a myriad
of ECG findings. These may include normal ECGs, nonspecific
T-wave inversions, ST depression, or transient ST elevation.
Treatment
Medical Therapy
Initial medical therapy for ACS includes rapid delivery of an-
tiplatelet agents, anticoagulants and revascularization therapy
to include fibrinolytic therapy (if no contraindications exist
and PCI is not immediately available). The below sections in-
clude lists of common available medications in each class.
Antiplatelet Therapy
Aspirin should be administered immediately to all patients with
suspected ACS if no contraindications exist. Once the diagnosis
of ACS has been made, a platelet adenosine diphosphate receptor
(P2Y) should be administered. An inhibitor (e.g., clopidogrel,
12
ticagrelor) should then also be administered if no contraindica-
tions exist. Initial dosing for all agents is listed below.
Similarly, if the initial ECG shows evidence of an inferior
STEMI (ST elevation in leads II, III, and aVF with reciprocal 1. Aspirin 162–325mg PO × 1 (chewable is preferred, non–
changes), then consider placing leads V –V on the patient as enteric coated preferred if chewable not available) then
6
1
a complete mirror reflection (as shown in Figure 14). If these 81mg PO daily.
leads (now called V R–V R) show ST elevation, this will be
1
6
consistent with right ventricular infarction. AND
14 | JSOM Volume 21, Edition 3 / Fall 2021