
Page 33 - JSOM Spring 2021
P. 33
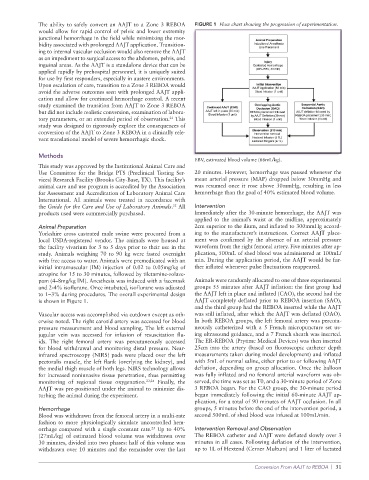
The ability to safely convert an AAJT to a Zone 3 REBOA FIGURE 1 Flow chart showing the progression of experimentation.
would allow for rapid control of pelvic and lower extremity
junctional hemorrhage in the field while minimizing the mor-
bidity associated with prolonged AAJT application. Transition-
ing to internal vascular occlusion would also remove the AAJT
as an impediment to surgical access to the abdomen, pelvis, and
inguinal areas. As the AAJT is a standalone device that can be
applied rapidly by prehospital personnel, it is uniquely suited
for use by first responders, especially in austere environments.
Upon escalation of care, transition to a Zone 3 REBOA would
avoid the adverse outcomes seen with prolonged AAJT appli-
cation and allow for continued hemorrhage control. A recent
study examined the transition from AAJT to Zone 3 REBOA
but did not include realistic conversion, examination of labora-
tory parameters, or an extended period of observation. This
21
study was designed to rigorously explore the consequences of
conversion of the AAJT to Zone 3 REBOA in a clinically rele-
vant translational model of severe hemorrhagic shock.
Methods
EBV, estimated blood volume (66mL/kg).
This study was approved by the Institutional Animal Care and
Use Committee for the Bridge PTS (Preclinical Testing Ser- 20 minutes. However, hemorrhage was paused whenever the
vices) Research Facility (Brooks City-Base, TX). This facility’s mean arterial pressure (MAP) dropped below 30mmHg and
animal care and use program is accredited by the Association was resumed once it rose above 30mmHg, resulting in less
for Assessment and Accreditation of Laboratory Animal Care hemorrhage than the goal of 40% estimated blood volume.
International. All animals were treated in accordance with
the Guide for the Care and Use of Laboratory Animals. All Intervention
22
products used were commercially purchased. Immediately after the 30-minute hemorrhage, the AAJT was
applied to the animal’s waist at the midline, approximately
Animal Preparation 2cm superior to the ilium, and inflated to 300mmHg accord-
Yorkshire cross castrated male swine were procured from a ing to the manufacturer’s instructions. Correct AAJT place-
local USDA-registered vendor. The animals were housed at ment was confirmed by the absence of an arterial pressure
the facility vivarium for 3 to 5 days prior to their use in the waveform from the right femoral artery. Five minutes after ap-
study. Animals weighing 70 to 90 kg were fasted overnight plication, 500mL of shed blood was administered at 100mL/
with free access to water. Animals were premedicated with an min. During the application period, the AAJT would be fur-
initial intramuscular (IM) injection of 0.02 to 0.05mg/kg of ther inflated whenever pulse fluctuations reappeared.
atropine for 15 to 30 minutes, followed by tiletamine-zolaze-
pam (4–8mg/kg IM). Anesthesia was induced with a facemask Animals were randomly allocated to one of three experimental
and 2-4% isoflurane. Once intubated, isoflurane was adjusted groups 55 minutes after AAJT inflation: the first group had
to 1–3% during procedures. The overall experimental design the AAJT left in place and inflated (CAO), the second had the
is shown in Figure 1. AAJT completely deflated prior to REBOA insertion (SAO),
and the third group had the REBOA inserted while the AAJT
Vascular access was accomplished via cutdown except as oth- was still inflated, after which the AAJT was deflated (OAO).
erwise noted. The right carotid artery was accessed for blood In both REBOA groups, the left femoral artery was percuta-
pressure measurement and blood sampling. The left external neously catheterized with a 5 French micropuncture set us-
jugular vein was accessed for infusion of resuscitation flu- ing ultrasound guidance, and a 7 French sheath was inserted.
ids. The right femoral artery was percutaneously accessed The ER-REBOA (Prytime Medical Devices) was then inserted
for blood withdrawal and monitoring distal pressure. Near- 25cm into the artery (based on fluoroscopic catheter depth
infrared spectroscopy (NIRS) pads were placed over the left measurements taken during model development) and inflated
pectoralis muscle, the left flank (overlying the kidney), and with 5mL of normal saline, either prior to or following AAJT
the medial thigh muscle of both legs. NIRS technology allows deflation, depending on group allocation. Once the balloon
for increased noninvasive tissue penetration, thus permitting was fully inflated and no femoral arterial waveform was ob-
monitoring of regional tissue oxygenation. 23,24 Finally, the served, the time was set as T0, and a 30-minute period of Zone
AAJT was pre-positioned under the animal to minimize dis- 3 REBOA began. For the CAO group, the 30-minute period
turbing the animal during the experiment. began immediately following the initial 60-minute AAJT ap-
plication, for a total of 90 minutes of AAJT occlusion. In all
Hemorrhage groups, 5 minutes before the end of the intervention period, a
Blood was withdrawn from the femoral artery in a multi-rate second 500mL of shed blood was infused at 100mL/min.
fashion to more physiologically simulate uncontrolled hem-
orrhage compared with a single constant rate. Up to 40% Intervention Removal and Observation
25
(27mL/kg) of estimated blood volume was withdrawn over The REBOA catheter and AAJT were deflated slowly over 3
30 minutes, divided into two phases: half of this volume was minutes in all cases. Following deflation of the intervention,
withdrawn over 10 minutes and the remainder over the last up to 1L of Hextend (Cerner Multum) and 1 liter of lactated
Conversion From AAJT to REBOA | 31