
Page 82 - JSOM Summer 2020
P. 82
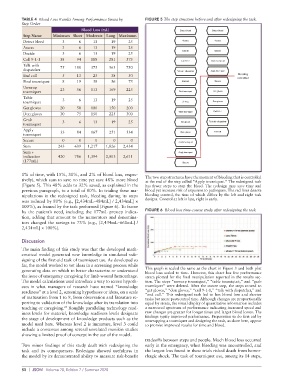
TABLE 4 Blood Loss Results Among Performance Strata by FIGURE 5 The step structure before and after redesigning the task.
Step Order
Blood Loss (mL) Detect bleed Detect bleed
Step Name Minimum Short Moderate Long Maximum
Detect bleed 3 6 13 19 25 Assess Assess
Assess 3 6 13 19 25
Decide Decide
Decide 3 6 13 19 25
Call 9-1-1 38 94 188 281 375
Call 9-1-1 Grab tourniquet
Talk with 75 188 375 563 750
dispatcher
Talk with dispatcher Apply tourniquet
End call 5 13 25 38 50 Bleeding
controlled
Find tourniquet 8 19 38 56 75 End call Secure
Unwrap
tourniquet 23 56 113 169 225 Find tourniquet Get gloves
Table
tourniquet 3 6 13 19 25 Unwrap Don gloves
Get gloves 20 50 100 150 200
Don gloves 30 75 150 225 300 Table tourniquet Call 9-1-1
Grab 3 6 13 19 25
tourniquet Get gloves Talk with dispatcher
Apply
tourniquet 33 84 167 251 334 Don gloves End call
Secure 0 0 0 0 0
Grab tourniquet
Sum 243 609 1,217 1,826 2,434
Sum + Apply tourniquet
indication 420 786 1,394 2,003 2,611
(177mL)
Secure
1% of time, with 15%, 31%, and 2% of blood loss, respec-
tively), which sum to save no time yet save 48% more blood The two step structures have the moment of bleeding that is controlled
at the end of the step called “Apply tourniquet.” The redesigned task
(Figure 5). This 48% adds to 32% saved, as explained in the has fewer steps to stop the bleed. The redesign may save time and
previous paragraph, to a total of 80%. In trialing these ma- blood yet increase risk of exposure to pathogens. The red lines denote
nipulations in the redesigned task, bleeding during its steps bleeding control, the time of which differs by the left and right task
was reduced by 80% (e.g., [2,434mL–484mL] / 2,434mL] × designs. Control at left is late, right is early.
100%), as framed by the task performed (Figure 6). To frame
by the patient’s need, including the 177mL prestep indica- FIGURE 6 Blood loss time-course study after redesigning the task
tion, adding that amount to the numerators and denomina-
tors changed the savings to 73% (e.g., [2,434mL–661mL] /
2,434mL] × 100%).
Discussion
The main finding of this study was that the developed math-
ematical model generated new knowledge in simulated rede-
signing of the first-aid task of tourniquet use. As developed so
far, the model worked to vet ideas in a screening process while
generating data on which to better characterize or understand This graph is scaled the same as the chart in Figure 3 and both plot
blood loss scaled to time. However, this chart has five performance
the issue of emergency caregiving for limb-wound hemorrhage. strata plotted for the final manipulation reported in the results sec-
The model calculations used introduce a way to screen hypoth- tion. The steps “unwrap tourniquet,” “table tourniquet,” and “grab
eses in what managers of research have named “knowledge tourniquet” were deleted. After the secure step, the steps moved to
readiness” at a level 2, screening hypotheses or ideas, on a scale “get gloves,” “don gloves,” “call 9-1-1,” “talk with dispatcher,” and
of maturation from 1 to 9, from observation and literature re- “end call.” This redesigned task led to less blood loss and shorter
tasks but more postcontrol time. Although changes are proportionally
porting to validation of the knowledge after its translation into equal by strata, the visual display of quantitative information includes
27
teaching or caregiving. Roughly paralleling technology read- a narrowed spectrum of performance indicating increased speed and
iness levels for materiel, knowledge readiness levels designate raw changes are greater for longer times and larger blood losses. The
the stage of development of knowledge products such as the findings typify improved performance. Preparation to do first aid by
unwrapping a tourniquet and designing the task, as done here, appear
model used here. Whereas level 2 is immature, level 3 could to promise improved results for time and blood.
include a consensus among several unrelated manikin studies
showing a limited proof of concept in the use of the model.
tradeoffs between steps and people. Much blood loss occurred
Two minor findings of this study dealt with redesigning the early in the emergency, when bleeding was uncontrolled, and
task and its consequences. Redesigns showed usefulness in the largest loss found in these trials risked death from hemor-
the model by its demonstrated ability to measure risk-benefit rhagic shock. The task of tourniquet use, among its 14 steps,
80 | JSOM Volume 20, Edition 2 / Summer 2020