
Page 91 - JSOM Summer 2019
P. 91
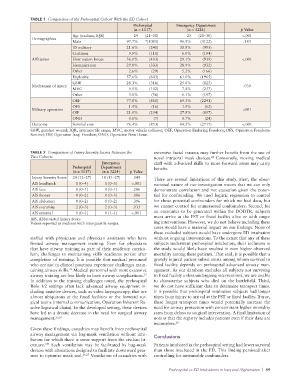
TABLE 1 Comparison of the Prehospital Cohort With the ED Cohort
Prehospital Emergency Department
(n = 1117) (n = 3224) p Value
Age (median, IQR) 24 (21–30) 25 (21–30) <.001
Demographics
Male 97.7% *(1091) 96.9% (3122) .183
US military 21.6% (241) 30.8% (993)
Coalition 9.9% (111) 6.0% (194)
Affiliation Host nation forces 36.1% (403) 29.1% (939) <.001
Humanitarian 29.8% (333) 28.9% (932)
Other 2.6% (29) 5.2% (166)
Explosive 57.6% (643) 61.0% (1965)
GSW 28.3% (316) 25.6% (825)
Mechanism of injury .030
MVC 9.1% (102) 7.4% (237)
Other 5.0% (56) 6.1% (197)
OEF 77.0% (860) 69.5% (2241)
OFS 1.4% (16) 1.9% (62)
Military operation <001
OIF 21.0% (234) 27.8% (897)
OND 0.6% (7) 0.7% (24)
Outcome Survival rate 76.4% (853) 84.3% (2717) <.001
GSW, gunshot wound; IQR, interquartile range; MVC, motor vehicle collision; OEF, Operation Enduring Freedom; OFS, Operation Freedoms
Sentinel; OIF, Operation Iraqi Freedom; OND, Operation New Dawn.
TABLE 2 Comparison of Injury Severity Scores Between the extensive facial trauma may further benefit from the use of
Two Cohorts novel intraoral mask devices. Conversely, moving medical
28
Emergency staff with advanced skills to more forward areas may carry
Prehospital Department benefit.
(n = 1117) (n = 3224) p Value
Injury Severity Score 20 (12–27) 18 (11–27) .045 There are several limitations of this study. First, the obser-
AIS head/neck 1 (0–4) 1 (0–3) <.001 vational nature of our investigation means that we can only
AIS face 0 (0–1) 0 (0–1) .286 demonstrate correlation and not causation given the poten-
AIS thorax 0 (0–2) 0 (0–3) .006 tial for confounding. We used logistic regression to control
AIS abdomen 0 (0–2) 0 (0–2) .396 for those potential confounders for which we had data, but
AIS extremity 2 (0–3) 2 (0–3) .033 we cannot control for unmeasured confounders. Second, for
AIS external 1 (0–1) 1 (1–1) <.001 an encounter to be generated within the DODTR, subjects
AIS, Abbreviated Injury Score. must arrive at the FST or fixed facility alive or with ongo-
Values reported as medians with interquartile ranges. ing interventions. However, we do not believe including these
cases would have a material impact on our findings. None of
these excluded subjects would have undergone ED intubation
staffed with physicians and physician assistants who have without ongoing interventions. To the extent that any of these
limited airway management training. Even for physicians subjects underwent prehospital intubation, their inclusion in
that have airway training as part of their residency curricu- the study would likely have resulted in even higher observed
lum, challenges to maintaining skills readiness persist after mortality among these patients. That said, it is possible that a
completion of training. It is possible that medical personnel gravely injured patient subset exists among whom survival to
who are not in clinical positions experience challenges main- fixed facility depends on prehospital advanced airway man-
22
taining airway skills. Medical personnel with more extensive agement. As our database excludes all subjects not surviving
15
airway training are less likely to have airway complications. to fixed facility unless undergoing interventions, we are unable
In addition to the training challenges noted, the prehospital to characterize subjects who died on the battlefield. Third,
Role 1/2 settings often lack advanced airway equipment in- we do not have sufficient data to determine transport times.
cluding assistive devices, such as video laryngoscopy, that are It is possible that prehospital intubation subjects had longer
almost ubiquitous at the fixed facilities or the forward sur- times from injury to arrival at the FST or fixed facility. If true,
gical teams (internal communication, Operation Inherent Re- these longer transport times would potentially increase the
solve logistical chain). In the developed setting, these devices need for airway protection with concomitant higher mortality
have led to a drastic decrease in the need for surgical airway rates from delays to surgical intervention. A final limitation of
management. 23,24 note is that the registry includes patients even if their data are
incomplete. 29
Given these findings, casualties may benefit from prehospital
airway management via bag-mask ventilation without intu- Conclusions
bation for which there is some support from the civilian lit-
254
erature. Such ventilation may be facilitated by bag-mask Patients intubated in the prehospital setting had lower survival
devices with alterations designed to facilitate downward pres- than those intubated in the ED. This finding persisted after
sure to optimize mask seal. 26,27 Ventilation of casualties with controlling for measurable confounders.
Prehospital vs ED Intubations in Iraq and Afghanistan | 89