
Page 95 - JSOM Summer 2019
P. 95
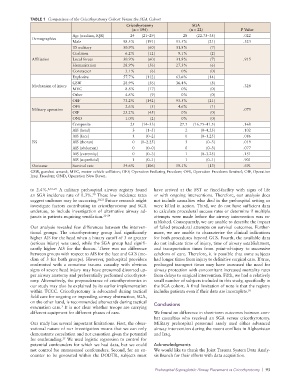
TABLE 1 Comparison of the Cricothyrotomy Cohort Versus the SGA Cohort
Cricothyrotomy SGA
(n = 194) (n = 22) P Value
Age (median, IQR) 24 (21–29) 28 (22.75–35) .022
Demographics
Male 98.5% (191) 95.5% (21) .323
US military 30.9% (60) 31.8% (7)
Coalition 6.2% (12) 9.1% (2)
Affiliation Local forces 30.9% (60) 31.8% (7) .915
Humanitarian 28.9% (56) 27.3% (6)
Contractor 3.1% (6) 0% (0)
Explosive 57.7% (112) 63.6% (14)
GSW 28.9% (56) 36.4% (8)
Mechanism of injury .328
MVC 8.8% (17) 0% (0)
Other 4.6% (9) 0% (0)
OEF 73.2% (142) 95.5% (21)
OFS 2.6% (5) 4.6% (1)
Military operation .075
OIF 23.2% (45) 0% (0)
OND 1.0% (2) 0% (0)
Composite 25 (14–33) 27.5 (16.75–41.5) .168
AIS (head) 3 (1–5) 2 (0–4.25) .102
AIS (face) 1 (0–2) 0 (0–1.25) .086
ISS AIS (thorax) 0 (0–2.25) 3 (0–3) .019
AIS (abdomen) 0 (0–0) 0 (0–3) .077
AIS (extremity) 0 (0–3) 1 (0–3.25) .151
AIS (superficial) 1 (0–1) 1 (0–1) .901
Outcome Survival rate 54.6% (106) 59.1% (13) .691
GSW, gunshot wound; MVC, motor vehicle collision; OEF, Operation Enduring Freedom; OFS, Operation Freedoms Sentinel; OIF, Operation
Iraqi Freedom; OND, Operation New Dawn.
to 2.4%. 4,16–21 A military prehospital airway registry found have arrived at the FST or fixed-facility with signs of life
an SGA incidence rate of 0.3%. These low incidence rates or with ongoing interventions. Therefore, our analysis does
20
suggest underuse may be occurring. 20,21 Future research might not include casualties who died in the prehospital setting or
investigate factors contributing to cricothyrotomy and SGA were killed in action. Third, we do not have sufficient data
underuse, to include investigation of alternative airway ad- to calculate procedural success rates or determine if multiple
juncts in patients requiring ventilation. 22–24 attempts were made before the airway intervention was es-
tablished. Consequently, we are unable to describe the impact
Our analysis revealed few differences between the interven- of failed procedural attempts on survival outcomes. Further-
tional groups. The cricothyrotomy group had significantly more, we are unable to characterize the clinical indications
higher AIS for the head when a binary cutoff of 3 or greater for both procedures beyond GCS. Fourth, the available data
(serious injury) was used, while the SGA group had signifi- do not indicate time of injury, time of airway establishment,
cantly higher AIS for the thorax. There was no difference and transportation times from point-of-injury to successive
between groups with respect to AIS for the face and GCS (me- echelons of care. Therefore, it is possible that some subjects
dian of 3 for both groups). However, prehospital providers had longer times from injury to definitive surgical care. If true,
confronted with a comatose trauma casualty with obvious prolonged transport times may have increased the need for
signs of severe head injury may have presumed distorted up- airway protection with concomitant increased mortality rates
per airway anatomy and preferentially performed cricothyrot- from delays to surgical intervention. Fifth, we had a relatively
omy. Alternatively, the preponderance of cricothyrotomies in small number of subjects included in this study, specifically in
our study may also be explained by its earlier implementation the SGA cohort. A final limitation of note is that the registry
within TCCC. Cricothyrotomy is advocated during tactical includes patients even if their data are incomplete. 26
field care for ongoing or impending airway obstruction; SGA,
on the other hand, is recommended afterwards during tactical Conclusions
evacuation care. It is not clear whether troops are carrying
3
different equipment for different phases of care. We found no difference in short-term outcomes between com-
bat casualties who received an SGA versus cricothyrotomy.
Our study has several important limitations. First, the obser- Military prehospital personnel rarely used either advanced
vational nature of our investigation means that we can only airway intervention during the recent conflicts in Afghanistan
demonstrate correlation and not causation given the potential and Iraq.
for confounding. We used logistic regression to control for
25
potential confounders for which we had data, but we could Acknowledgments
not control for unmeasured confounders. Second, for an en- We would like to thank the Joint Trauma System Data Analy-
counter to be generated within the DODTR, subjects must sis Branch for their efforts with data acquisition.
Prehospital Supraglottic Airway Placement vs Cricothyrotomy | 93