
Page 136 - JSOM Summer 2018
P. 136
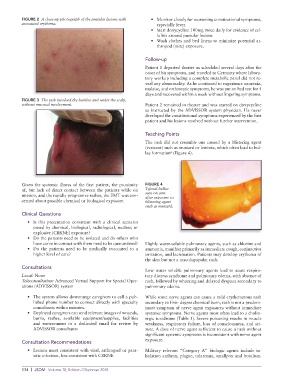
FIGURE 2 A close-up photograph of the pustular lesions with • Monitor closely for worsening constitutional symptoms,
associated erythema. especially fever.
• Start doxycycline 100mg twice daily for evidence of cel-
lulitis around pustular lesions
• Wash clothes and bed linens to minimize potential ar-
thropod (mite) exposure.
Follow-up
Patient 1 departed theater as scheduled several days after the
onset of his symptoms, and traveled to Germany where labora-
tory workup including a complete metabolic panel did not re-
veal any abnormality. As he continued to experience anorexia,
malaise, and orthostatic symptoms, he was put on bed rest for 5
days and recovered within a week without lingering symptoms.
FIGURE 3 The rash involved the hairline and under the scalp,
without mucosal involvement. Patient 2 remained in theater and was started on doxycycline
as instructed by the ADVISSOR system physician. He never
developed the constitutional symptoms experienced by the first
patient and his lesions resolved without further intervention.
Teaching Points
The rash did not resemble one caused by a blistering agent
(vesicant) such as mustard or lewisite, which often lead to bul-
lae formation (Figure 4).
6
Given the systemic illness of the first patient, the proximity FIGURE 4
of, but lack of direct contact between the patients while on Typical bullae
mission, and the rapidly progressive rashes, the EMT was con- seen on arm
after exposure to
cerned about possible chemical or biological exposure. blistering agent
such as mustard.
Clinical Questions
• Is this presentation consistent with a clinical scenario
posed by chemical, biological, radiological, nuclear, or
explosive (CBRNE) exposure?
• Do the patients need to be isolated and do others who
have come in contact with them need to be quarantined? Highly water-soluble pulmonary agents, such as chlorine and
• Do the patients need to be medically evacuated to a ammonia, manifest primarily as immediate cough, conjunctiva
higher level of care? irritation, and lacrimation. Patients may develop erythema of
the skin but not a maculopapular rash.
Consultations
Low water soluble pulmonary agents lead to acute respira-
Local: None tory distress syndrome and pulmonary edema, with absence of
Teleconsultation: Advanced Virtual Support for Special Oper- rash, followed by wheezing and delayed dyspnea secondary to
ations (ADVISSOR) system pulmonary edema.
• The system allows downrange caregivers to call a pub- While some nerve agents can cause a mild erythematous rash
lished phone number to connect directly with specialty secondary to first- degree chemical burn, rash is not a predom-
consultants within minutes. inant symptom of nerve agent exposures without immediate
• Deployed caregivers can send relevant images of wounds, systemic symptoms. Nerve agents most often lead to a cholin-
burns, rashes, available equipment/supplies, facilities ergic toxidrome (Table 1). Severe poisoning results in muscle
and environment to a dedicated email for review by weakness, respiratory failure, loss of consciousness, and sei-
ADVISSOR consultants zure. A dose of nerve agent sufficient to cause a rash without
significant systemic symptoms is inconsistent with nerve agent
exposure.
Consultation Recommendations
• Lesions most consistent with viral, arthropod or para- Military relevant “Category A” biologic agents include in-
sitic infection, less consistent with CBRNE halation anthrax, plague, tularemia, smallpox and botulism.
134 | JSOM Volume 18, Edition 2/Summer 2018