
Page 34 - JSOM Spring 2018
P. 34
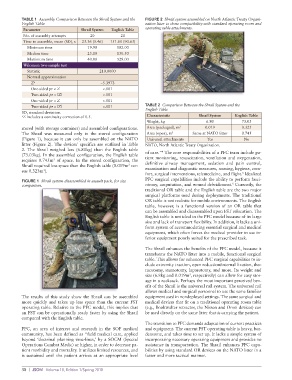
TABLE 1 Assembly Comparison Between the Shrail System and the FIGURE 2 Shrail system assembled on North Atlantic Treaty Organi-
English Table zation litter to show compatibility with standard operating room and
Parameter Shrail System English Table operating table attachments.
No. of assembly attempts 20 20
Time to assemble, mean (SD), s 23.36 (5.46) 151.60 (90.63)
Minimum time 19.90 102.00
Median time 25.10 130.50
Maximum time 40.00 528.00
Wilcoxon two-sample test
Statistic 210.0000
Normal approximation
Z a −5.3973
One-sided pr < Z <.001
Two-sided pr > |Z| <.001
One-sided pr < Z <.001
Two-sided pr > |Z| <.001 TABLE 2 Comparison Between the Shrail System and the
English Table
SD, standard deviation.
a Z includes a continuity correction of 0.5. Characteristic Shrail System English Table
Weight, kg 6.80 73.03
stored (with storage container) and assembled configurations. Area (packaged), m 3 0.019 0.323
The Shrail was measured only in the stored configuration Area (open), m 3 Same at NATO litter 0.745
(Figure 1), because it can only be assembled on the NATO Universal attachments Yes No
litter (Figure 2). The devices’ specifics are outlined in Table NATO, North Atlantic Treaty Organization.
2. The Shrail weighed less (6.80kg) than the English table 4
(73.03kg). In the assembled configuration, the English table of care.” The core responsibilities of a PFC team include pa-
3
requires 0.745m of space. In the stored configuration, the tient monitoring, resuscitation, ventilation and oxygenation,
Shrail required less space than the English table (0.019m ver- definitive airway management, sedation and pain control,
3
sus 0.323m ). examination and diagnostic measures, nursing, hygiene, com-
3
fort, surgical interventions, telemedicine, and flight. Idealized
5
FIGURE 1 Shrail system disassembled in assault pack, for size PFC surgical capabilities include the ability to perform fasci-
5
comparison. otomy, amputation, and wound debridement. Currently, the
traditional OR table and the English table are the two major
surgical platforms used during deployments. The traditional
OR table is not realistic for mobile environments. The English
table, however, is a functional version of an OR table that
can be assembled and disassembled upon FST relocation. The
English table is not ideal in the PFC model because of its large
size and lack of transport flexibility. In addition, it lacks a uni-
form system of accommodating essential surgical and medical
equipment, which often forces the medical provider to use in-
ferior equipment poorly suited for the prescribed task.
The Shrail enhances the benefits of the PFC model, because it
transforms the NATO litter into a mobile, functional surgical
table. This allows for enhanced PFC surgical capabilities to in-
clude extremity traction, open reduction/internal fixation, tho-
racotomy, sternotomy, laparotomy, and more. Its weight and
3
size (6.8kg and 0.019m , respectively) can allow for easy stor-
age in a rucksack. Perhaps the most important perceived ben-
efit of the Shrail is the universal rail system. The universal rail
allows medical and surgical personnel to use the same familiar
The results of this study show the Shrail can be assembled equipment used in nondeployed settings. The same surgical and
more quickly and takes up less space than the current FST medical devices that fit on a traditional operating room table
operating table. Relative to the PFC model, this implies that (e.g., Bookwalter retractor, the Nissen and Omni devices) can
an FST can be operationally ready faster by using the Shrail be used directly on the same litter that is carrying the patient.
compared with the English table.
The transition to PFC demands adaptation of current practices
PFC, an area of interest and research in the SOF medical and equipment. The current FST operating table is heavy, bur-
community, has been defined as “field medical care, applied densome, and takes time to set up. It lacks a simple system of
beyond ‘doctrinal planning time-lines,’ by a SOCM (Special incorporating necessary operating equipment and provides no
Operations Combat Medic) or higher, in order to decrease pa- assistance in transportation. The Shrail enhances PFC capa-
tient morbidity and mortality. It utilizes limited resources, and bilities by using standard OR devices on the NATO litter in a
is sustained until the patient arrives at an appropriate level faster and more tactical manner.
30 | JSOM Volume 18, Edition 1/Spring 2018