
Page 143 - JSOM Spring 2018
P. 143
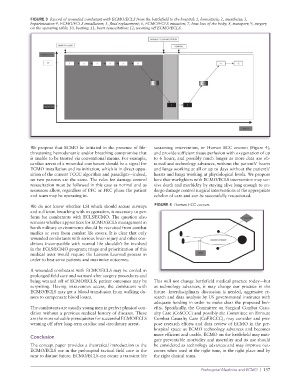
FIGURE 3 Record of wounded combatant with ECMO/ECLS from the battlefield to the hospital: 1, hemostasis; 2, anesthesia; 3,
heparinization 4, ECMO/ECLS installation; 5, fluid replacement; 6, ECMO/ECLS initiation; 7, heat loss of the body; 8, transport; 9, surgery
on the operating table; 10, heating; 11, heart resuscitation; 12, weaning off ECMO/ECLS.
We propose that ECMO be initiated in the presence of life- sustaining intervention, or Human ECC cocoon (Figure 4),
threatening hemodynamic and/or breathing compromise that and provide sufficient tissue perfusion with oxygenation of up
is unable to be treated via conventional means. For example, to 6 hours, and possibly much longer as more data are ob-
cardiac arrest of a wounded combatant should be a signal for tained and technology advances, without the patient’s’ hearts
ECMO installation and its initiation, which is in direct oppo- and lungs working at all or up to days without the patient’s’
sition of the current TCCC algorithm and paradigm—indeed, hearts and lungs working at physiological levels. We propose
no two patients are the same. The rules for damage control here that warfighters with ECMO/ECLS intervention may sur-
resuscitation must be followed in this case as normal and as vive death and morbidity by staying alive long enough to un-
resources allow, regardless of PFC or FRC phase the patient dergo damage control surgical interventions at the appropriate
and team may be operating in. echelon of care and can be successfully resuscitated.
We do not know whether LSI which should secure airways FIGURE 4 Human ECC cocoon.
and sufficient breathing with oxygenation, is necessary to per-
form for combatants with ECLS/ECMO. The question also
remains whether apprentices for ECMO/ECLS management in
harsh military environments should be recruited from combat
medics or even from combat life savers. It is clear that only
wounded combatants with serious brain injury and other con-
ditions incompatible with normal life shouldn’t be involved
in the ECLS/ECMO program; triage and prioritization of this
medical asset would require the Lessons Learned process in
order to best serve patients and maximize outcomes.
A wounded combatant with ECMO/ECLS may be cooled in
prolonged field care and warmed after surgery procedures and
being weaned off of ECMO/ECLS; patient outcomes may be This will not change battlefield medical practice today—but
surprising. Having intravenous access, the combatant with as technology advances, it may change our practice in the
ECMO/ECLS may get a blood transfusion from walking do- future. Interdisciplinary discussion is needed, aggressive re-
nors to compensate blood losses. search and data analysis by US governmental institutes with
adequate funding in order to make clear the proposed ben-
The combatants are usually young men in perfect physical con- efits. Specifically, the Committee on Surgical Combat Casu-
dition without a previous medical history of diseases. These alty Care (CoSCCC) and possibly the Committee on Enroute
are the most valuable prerequisites for successful ECMO/ECLS Combat Casualty Care (CoERCCC), may consider and pro-
weaning off after long-term cardiac and circulatory arrest. pose research efforts and data review of ECMO in the pre-
hospital space as ECMO technology advances and becomes
more efficient and usable. ECMO on the battlefield may miti-
Conclusion
gate preventable morbidity and mortality and its use should
The concept paper provides a theoretical introduction to the be considered as technology advances and may improve out-
ECMO/ECLS use in the prehospital tactical field care in the comes when used at the right time, in the right place and by
near to distant future. ECMO/ECLS can create a transient life the right clinical team.
Prehospital Medicine and ECMO | 137