
Page 19 - JSOM Spring 2026
P. 19
medical operations, supporting the Battalion Medical Officers The Role 2 surgical platoon’s officer in charge (OIC) coordi-
and ensuring that casualties are evacuated efficiently through nated with the Role 1 units and medical coordination cell via
the echelons of care. The Role 2 surgical company works TAK. Role 2 physicians communicated directly with Role 1
closely with Regimental Role 1 units ensuring effective casu- providers, optimizing treatment plans through real-time text,
alty evacuation and care, especially in amphibious operations photos, and videos. For example, when a wave of casualties
or other complex missions. 9,10 These units coordinate closely was reported 40 minutes inbound via TAK, the medical teams
to manage casualties through the continuum of care, ensuring were able to prepare equipment and blood products in ad-
they receive the right level of care at the right time (Figure 1). vance. In a second wave, the Role 2 facility became mission-in-
capable due to flooding. The Role 1 team, 30 minutes away,
USMC communication systems primarily support fire support received a critically injured patient requiring surgical care. The
and command, but medical information is often less opti- trauma surgeon, in real-time via TAK, advised the Role 1 team
mized. With TAK, medical units can share detailed information to declare the patient expectant to conserve resources (Appen-
within the USMC communications framework, enabling the dix A).
creation of a de facto medical control (MEDCON) chain from
corpsmen to high-level medical commands like the Marine Ex- Exercise #2 (November 2022):
peditionary Force (MEF) Surgeon cell. This network ensures Keen Sword 23 exercise was a large bilateral military exercise
rapid, efficient communication, allowing medical personnel to between the U.S. Military and the Japanese Self Defense Force.
quickly request additional resources and support across the III MEF conducted distributed Joint and Combined maritime
JTS as needed. operations across the First Island Chain (FIC) with the Japan
Ground Self-Defense Force. TAK was employed to coordi-
Evaluation of TAK in Support of nate casualty care across a 150 nautical mile area, including a
Health Services Support Operations forward-deployed Role 1 BAS, mobile ERCs, a Role 2 surgical
platoon, and a Role 3 US Navy (USN) Expeditionary Medical
Exercise #1 (July 2022): Facility (EMF).
During this exercise in the Republic of Korea, a III MEF en-
gineering battalion was reinforced with various medical el- During this exercise, an ERC team was transporting patients
ements, including a Role 2 Damage Control Surgery (DCS) between Role 2 and Role 3 when their MV-22 Osprey made an
surgical platoon, Role 1 Damage Control Resuscitation (DCR) unplanned landing on a remote island. TAK allowed continu-
teams, a Role 1 BAS, Enroute Care Teams (ERCs), and a Pa- ous communication with the Role 2, Role 3, and line command
tient Evacuation Team (PET). TAK was used as the primary headquarters, enabling medical liaisons to inform the chain
communication tool across all units. Medical and non-medical of command of the situation before conventional communi-
personnel evaluated TAK’s ability to coordinate resources and cation channels. These exercises demonstrated TAK’s ability
casualty movement across a geographically dispersed area af- to streamline casualty tracking, improve communication, and
ter simulated attacks. support decision-making in dispersed, dynamic environments.
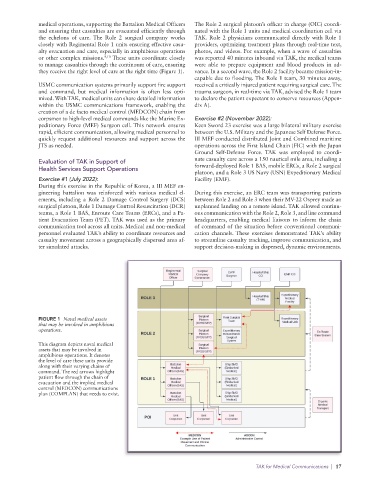
FIGURE 1 Naval medical assets
that may be involved in amphibious
operations.
This diagram depicts naval medical
assets that may be involved in
amphibious operations. It denotes
the level of care these units provide
along with their varying chains of
command. The red arrows highlight
patient flow through the chain of
evacuation and the implied medical
control (MEDCON) communications
plan (COMPLAN) that needs to exist.
TAK for Medical Communications | 17