
Page 63 - JSOM Winter 2025
P. 63
list any skills for ASM during “Circulation/Bleeding Control” This is another reason tourniquet reassessment should be at
as seen in Figure 2 below. the forefront of every soldier’s mind during all phases of ca-
sualty care.
FIGURE 2 Circulation/Bleeding Control, TCCC Skill Sets by
Responder Level Master List 2024. 16
Recommendations
Circulation / Bleeding Control ASM CLS CM/HM CP
Assessment and Treatment of 1. Tourniquet reassessment should be clearly reclassified as an
Bleeding in TCCC X X X ASM (Tier 1) skill.
Pelvic Compression Device 2. All service members should be trained to identify and re-
Application X X solve ineffective or not medically indicated tourniquets via
Tourniquet Reassessment / tourniquet conversion and tourniquet optimization within
Replacement X X X 2 hours of initial application.
Tourniquet Conversion to X X X 3. To emphasize these skills, TCCC training lanes should have
Other Hemostatic Adjuncts tourniquet reassessment and TC/TO as critical passing
criteria.
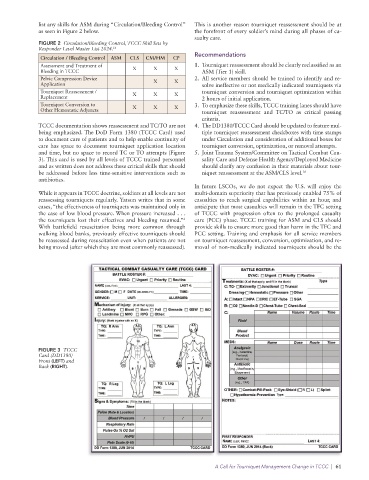
TCCC documentation shows reassessment and TC/TO are not 4. The DD1380/TCCC Card should be updated to feature mul-
being emphasized. The DoD Form 1380 (TCCC Card) used tiple tourniquet reassessment checkboxes with time stamps
to document care of patients and to help enable continuity of under Circulation and consideration of additional boxes for
care has space to document tourniquet application location tourniquet conversion, optimization, or removal attempts.
and time, but no space to record TC or TO attempts (Figure 5. Joint Trauma System/Committee on Tactical Combat Cau-
3). This card is used by all levels of TCCC trained personnel sality Care and Defense Health Agency/Deployed Medicine
and as written does not address these critical skills that should should clarify any confusion in their materials about tour-
be addressed before less time-sensitive interventions such as niquet reassessment at the ASM/CLS level. 16
antibiotics.
In future LSCOs, we do not expect the U.S. will enjoy the
While it appears in TCCC doctrine, soldiers at all levels are not multi-domain superiority that has previously enabled 75% of
reassessing tourniquets regularly. Yatsun writes that in some casualties to reach surgical capabilities within an hour, and
cases, “the effectiveness of tourniquets was maintained only in anticipate that most casualties will remain in the TFC setting
the case of low blood pressure. When pressure increased . . . of TCCC with progression often to the prolonged casualty
the tourniquets lost their effectives and bleeding resumed.” care (PCC) phase. TCCC training for ASM and CLS should
6
With battlefield resuscitation being more common through provide skills to ensure more good than harm in the TFC and
walking blood banks, previously effective tourniquets should PCC setting. Training and emphasis for all service members
be reassessed during resuscitation even when patients are not on tourniquet reassessment, conversion, optimization, and re-
being moved (after which they are most commonly reassessed). moval of non-medically indicated tourniquets should be the
FIGURE 3 TCCC
Card (DD1380)
Front (LEFT) and
Back (RIGHT).
A Call for Tourniquet Management Change in TCCC | 61