
Page 68 - JSOM Winter 2025
P. 68
• Commercial (210) 916-2876 or (210) 222-2876 o All patients with a burn size >20% TBSA will typically
• Email to usarmy.jbsa.medcom-aisr.list.armyburncenter@ need burn resuscitation. Some patients with 10%–19%
health.mil TBSA will need resuscitation.
6. Evacuating the patient to definitive care. o Best: Calculate burn resuscitation needs using the rule
of tens:
14
Burn Severity Calculation considerations include the – For adults weighing >40kg and <80kg, initial rate =
following: 10×TBSA.
• Best: After wounds are cleaned and debrided, recalculate – If >80kg, add 100mL/h for every 10kg >80kg.
TBSA using the Lund Browder chart available through the – Administer Lactated Ringer’s (LR) at a calculated
Burn Wound Management Under Prolonged Field Care rate: in this patient’s case, 32%×10=320mL/h. As the
CPG. 14 patient weighs 90kg, the total IV fluid rate should be
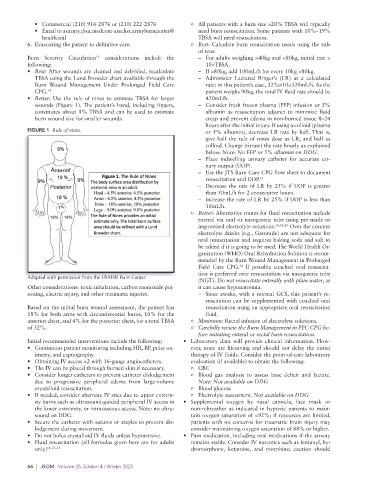
• Better: Use the rule of nines to estimate TBSA for larger 420mL/h.
wounds (Figure 1). The patient’s hand, including fingers, – Consider fresh frozen plasma (FFP) infusion or 5%
constitutes about 1% TBSA and can be used to estimate albumin as resuscitation adjunct to minimize fluid
burn wound size for smaller wounds. creep and prevent edema in non-burned tissue 8–24
hours after the initial injury. If using a colloid (plasma
FIGURE 1 Rule of nines. or 5% albumin), decrease LR rate by half. That is,
give half the rule of nines dose as LR, and half as
colloid. Change (titrate) the rate hourly as explained
below. Note: No FFP or 5% albumin on DDG.
– Place indwelling urinary catheter for accurate uri-
nary output (UOP).
– Use the JTS Burn Care CPG flow sheet to document
resuscitation and UOP. 15
– Decrease the rate of LR by 25% if UOP is greater
than 50mL/h for 2 consecutive hours.
– Increase the rate of LR by 25% if UOP is less than
30mL/h.
o Better: Alternative routes for fluid resuscitation include
enteral via oral or nasogastric tube using pre-made or
improvised electrolyte solutions. 14,18,19 Over the counter
electrolyte drinks (e.g., Gatorade) are not adequate for
oral resuscitation and requires baking soda and salt to
be added if it is going to be used. The World Health Or-
ganization (WHO) Oral Rehydration Solution is recom-
mended by the Burn Wound Management in Prolonged
Field Care CPG. If possible coached oral resuscita-
14
tion is preferred over resuscitation via nasogastric tube
Adapted with permission from the USAISR Burn Center.
(NGT). Do not resuscitate enterally with plain water, as
Other considerations: toxic inhalation, carbon monoxide poi- it can cause hyponatremia.
soning, electric injury, and other traumatic injuries. – Since awake, with a normal GCS, this patient’s re-
suscitation can be supplemented with coached oral
Based on the initial burn wound assessment, the patient has resuscitation using an appropriate oral resuscitation
18% for both arms with circumferential burns, 10% for the fluid.
anterior chest, and 4% for the posterior chest, for a total TBSA o Minimum: Rectal infusion of electrolyte solutions.
of 32%. o Carefully review the Burn Management in PFC CPG be-
fore initiating enteral or rectal burn resuscitation.
Initial recommended interventions include the following: • Laboratory data will provide clinical information. How-
• Continuous patient monitoring including HR, BP, pulse ox- ever, none are lifesaving and should not delay the initial
imetry, and capnography. therapy of IV fluids. Consider the point-of-care laboratory
• Obtaining IV access ×2 with 16-gauge angiocatheters. evaluation (if available) to obtain the following:
• The IV can be placed through burned skin if necessary. o CBC
• Consider longer catheters to prevent catheter dislodgement o Blood gas analysis to assess base deficit and lactate.
due to progressive peripheral edema from large-volume Note: Not available on DDG
crystalloid resuscitation. o Blood glucose
• If needed, consider alternate IV sites due to upper extrem- o Electrolyte assessment. Not available on DDG
ity burns such as ultrasound-guided peripheral IV access in • Supplemental oxygen by nasal cannula, face mask or
the lower extremity, or intraosseous access. Note: no ultra- non-rebreather as indicated in hypoxic patients to main-
sound on DDG. tain oxygen saturation of <92%; if resources are limited,
• Secure the catheter with sutures or staples to prevent dis- patients with no concerns for traumatic brain injury may
lodgement during movement. consider maintaining oxygen saturation of 88% or higher.
• Do not bolus crystalloid IV fluids unless hypotensive. • Pain medication, including oral medications if the airway
• Fluid resuscitation (all formulas given here are for adults remains stable. Consider IV narcotics such as fentanyl, hy-
only) 11,13–15 dromorphone, ketamine, and morphine; caution should
66 | JSOM Volume 25, Edition 4 / Winter 2025