
Page 71 - 2023 SMOG Digital
P. 71
Environmental
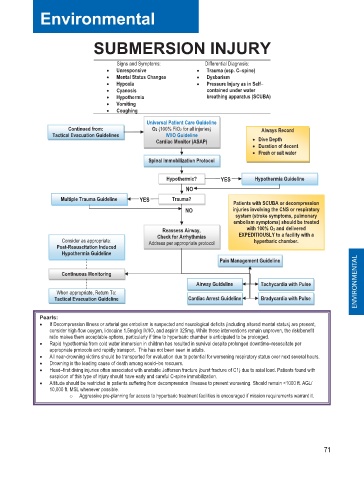
SUBMERSION INJURY
Signs and Symptoms: Differential Diagnosis:
• Unresponsive • Trauma (esp. C––spine)
• Mental Status Changes • Dysbarism
• Hypoxia • Pressure Injury as in Self– –
• Cyanosis contained under water
• Hypothermia breathing apparatus (SCUBA)
• Vomiting
• Coughing
Universal Patient Care Guideline
Continued from: O2 (100% FiO2 for all injuries) Always Record
Tactical Evacuation Guidelines IV/IO Guideline
Cardiac Monitor (ASAP) • Dive Depth
• Duration of decent
e
r
• F Fresh or salt water e r
t
l
a
t
a
w
h
s
o
s
r
Spinal Immobilization Protocol
Hypothermic? YES Hypothermia Guideline
NO
Multiple Trauma Guideline YES Trauma? Patients with SCUBA or decompression
NO injuries involving the CNS or respiratory
system (stroke symptoms, pulmonary
embolism symptoms) should be treated
Reassess Airway, with 100% O2 and delivered
Check for Arrhythmias EXPEDITIOUSLY to a facility with a
Consider as appropriate: Address per appropriate protocol hyperbaric chamber.
Post-Resuscitation Induced
Hypothermia Guideline
Pain Management Guideline
Continuous Monitoring
Airway Guideline Tachycardia with Pulse ENVIRONMENTAL
When appropriate, Return To:
Tactical Evacuation Guideline Cardiac Arrest Guideline Bradycardia with Pulse
Pearls:
• If Decompression Illness or arterial gas embolism is suspected and neurological deficits (including altered mental status) are present,
consider high-flow oxygen, lidocaine 1.5mg/kg IV/IO, and aspirin 325mg. While these interventions remain unproven, the risk/benefit
ratio makes them acceptable options, particularly if time to hyperbaric chamber is anticipated to be prolonged.
• Rapid hypothermia from cold water immersion in children has resulted in survival despite prolonged downtime–resuscitate per
appropriate protocols and rapidly transport. This has not been seen in adults.
• All near-drowning victims should be transported for evaluation due to potential for worsening respiratory status over next several hours.
• Drowning is the leading cause of death among would–be rescuers.
• Head–first diving injuries often associated with unstable Jefferson fracture (burst fracture of C1) due to axial load. Patients found with
suspicion of this type of injury should have early and careful C-spine immobilization.
• Altitude should be restricted in patients suffering from decompression illnesses to prevent worsening. Should remain <1000 ft. AGL/
10,000 ft. MSL whenever possible.
o Aggressive pre-planning for access to hyperbaric treatment facilities is encouraged if mission requirements warrant it.
71