
Page 65 - JSOM Spring 2023
P. 65
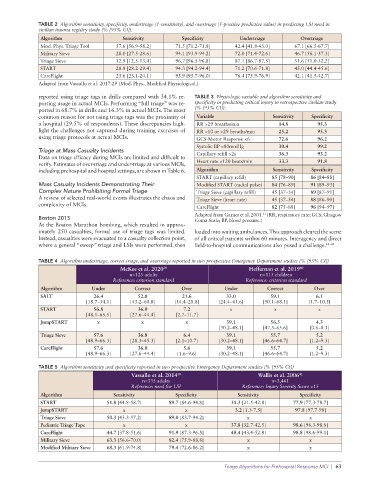
TABLE 2 Algorithm sensitivity, specificity, undertriage (1-sensitivity), and overtriage (1-positive predictive value) in predicting LSI need in
civilian trauma registry study (% [95% CI]).
Algorithm Sensitivity Specificity Undertriage Overtriage
Mod. Phys. Triage Tool 57.6 [56.9-58.2] 71.5 [71.2-71.8] 42.4 [41.8-43.0] 67.1 [66.5-67.7]
Military Sieve 28.0 [27.5-28.6] 94.1 [93.9-94.2] 72.0 [71.4-72.6] 46.7 [56.1-57.3]
Triage Sieve 12.9 [12.5-13.4] 96.7 [96.5-96.8] 87.1 [86.7-87.5] 51.6 [51.0-52.2]
START 28.8 [28.2-29.4] 94.3 [94.2-94.4] 71.2 [70.6-71.8] 45.0 [44.4-45.6]
CareFlight 23.6 [23.1-24.1] 95.9 [95.7-96.0] 76.4 [75.9-76.9] 42.1 [41.5-42.7]
Adapted from Vassallo et al. 2017.29 (Mod. Phys., Modified Physiological.)
reported using triage tags in drills compared with 34.1% re- TABLE 3 Physiologic variable and algorithm sensitivity and
porting usage in actual MCIs. Performing “full triage” was re- specificity in predicting critical injury in retrospective civilian study
ported in 68.7% in drills and 16.3% in actual MCIs. The most (% [95% CI]).
common reason for not using triage tags was the proximity of Variable Sensitivity Specificity
a hospital (29.5% of respondents). These discrepancies high- RR >29 breaths/min 14.8 95.3
light the challenges not captured during training exercises of RR <10 or >29 breaths/min 25.2 95.3
using triage protocols at actual MCIs. GCS-Motor Response <6 72.6 96.2
Systolic BP <80mmHg 30.4 99.2
Triage at Mass Casualty Incidents
Data on triage efficacy during MCIs are limited and difficult to Capillary refill >2s 36.3 93.2
verify. Estimates of over-triage and under-triage at various MCIs, Heart rate >120 beats/min 33.3 91.8
including prehospital and hospital settings, are shown in Table 6. Algorithm Sensitivity Specificity
START (capillary refill) 85 [78–90] 86 [84–88]
Mass Casualty Incidents Demonstrating Their Modified START (radial pulse) 84 [76–89] 91 [89–93]
Complex Nature Prohibiting Formal Triage Triage Sieve (capillary refill) 45 [37–54] 89 [87–91]
A review of selected real-world events illustrates the chaos and Triage Sieve (heart rate) 45 [37–54] 88 [86–90]
complexity of MCIs. CareFlight 82 [75–88] 96 [94–97]
Adapted from Garner et al. 2001. (RR, respiratory rate; GCS, Glasgow
21
Boston 2013 Coma Scale; BP, blood pressure.)
At the Boston Marathon bombing, which resulted in approx-
imately 250 casualties, formal use of triage tags was limited. loaded into waiting ambulances. This approach cleared the scene
Instead, casualties were evacuated to a casualty collection point, of all critical patients within 60 minutes. Interagency and direct
where a general “sweep” triage and LSIs were performed, then field-to-hospital communications also posed a challenge. 43–45
TABLE 4 Algorithm undertriage, correct triage, and overtriage reported in two prospective Emergency Department studies (% [95% CI])
McKee et al. 2020 39 Heffernan et al. 2019 40
n=125 adults n=115 children
Reference: criterion standard Reference: criterion standard
Algorithm Under Correct Over Under Correct Over
SALT 26.4 52.0 21.6 33.0 59.1 6.1
[18.7–34.1] [43.2–60.8] [14.4–28.8] [24.4–41.6] [50.1–68.1] [1.7–10.5]
START 56.8 36.0 7.2 x x x
[48.1–65.5] [27.6–44.4] [2.7–11.7]
JumpSTART x x x 39.1 56.5 4.3
[30.2–48.1] [47.5–65.6] [0.6–8.1]
Triage Sieve 57.6 36.8 6.4 39.1 55.7 5.2
[48.9–66.3] [28.3–45.3] [2.1–10.7] [30.2–48.1] [46.6–64.7] [1.2–9.3]
CareFlight 57.6 36.0 5.6 39.1 55.7 5.2
[48.9–66.3] [27.6–44.4] [1.6–9.6] [30.2–48.1] [46.6–64.7] [1.2–9.3]
TABLE 5 Algorithm sensitivity and specificity reported in two prospective Emergency Department studies (% [95% CI])
Vassallo et al. 2014 30 Wallis et al. 2006 41
n=335 adults n=3,461
Reference: need for LSI Reference: Injury Severity Score >15
Algorithm Sensitivity Specificity Sensitivity Specificity
START 51.8 [44.8-58.7] 89.7 [84.6-94.8] 31.3 [21.5-42.8] 77.9 [77.3-78.7]
JumpSTART x x 3.2 [1.3-7.5] 97.8 [97.7-98]
Triage Sieve 50.3 [43.3-57.2] 89.0 [83.7-94.2] x x
Pediatric Triage Tape x x 37.8 [32.7-42.5] 98.6 [98.3-98.8]
CareFlight 44.7 [37.8-51.6] 91.9 [87.3-96.5] 48.4 [43.4-52.8] 98.8 [98.6-99.1]
Military Sieve 63.3 [56.6-70.0] 82.4 [75.9-88.8] x x
Modified Military Sieve 68.3 [61.9-74.8] 79.4 [72.6-86.2] x x
Triage Algorithms for Prehospital Response MCI | 63