
Page 63 - JSOM Spring 2023
P. 63
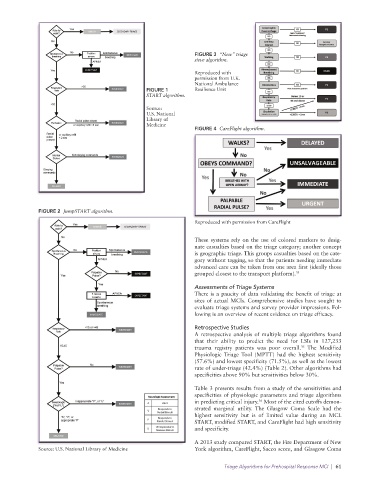
FIGURE 3 “New” triage
sieve algorithm.
Reproduced with
permission from U.K.
National Ambulance
FIGURE 1 Resilience Unit
START algorithm.
Source:
U.S. National
Library of
Medicine
FIGURE 4 CareFlight algorithm.
FIGURE 2 JumpSTART algorithm.
Reproduced with permission from CareFlight
These systems rely on the use of colored markers to desig-
nate casualties based on the triage category; another concept
is geographic triage. This groups casualties based on the cate-
gory without tagging, so that the patients needing immediate
advanced care can be taken from one area first (ideally those
grouped closest to the transport platform). 34
Assessments of Triage Systems
There is a paucity of data validating the benefit of triage at
sites of actual MCIs. Comprehensive studies have sought to
evaluate triage systems and survey provider impressions. Fol-
lowing is an overview of recent evidence on triage efficacy.
Retrospective Studies
A retrospective analysis of multiple triage algorithms found
that their ability to predict the need for LSIs in 127,233
trauma registry patients was poor overall. The Modified
35
Physiologic Triage Tool (MPTT) had the highest sensitivity
(57.6%) and lowest specificity (71.5%), as well as the lowest
rate of under-triage (42.4%) (Table 2). Other algorithms had
specificities above 90% but sensitivities below 30%.
Table 3 presents results from a study of the sensitivities and
specificities of physiologic parameters and triage algorithms
36
in predicting critical injury. Most of the cited cutoffs demon-
strated marginal utility. The Glasgow Coma Scale had the
highest sensitivity but is of limited value during an MCI.
START, modified START, and CareFlight had high sensitivity
and specificity.
A 2013 study compared START, the Fire Department of New
Source: U.S. National Library of Medicine York algorithm, CareFlight, Sacco score, and Glasgow Coma
Triage Algorithms for Prehospital Response MCI | 61