
Page 79 - JSOM Spring 2021
P. 79
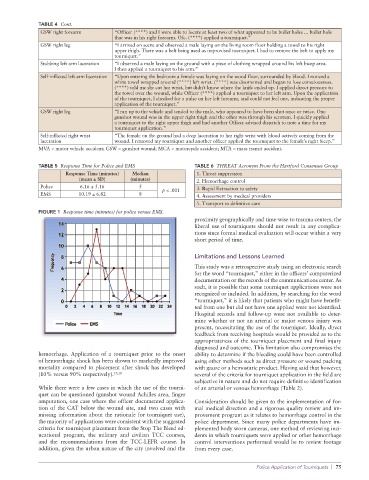
TABLE 4 Cont.
GSW right forearm “Officer (****) and I were able to locate at least two of what appeared to be bullet holes ... bullet hole
that was in his right forearm. Ofc. (****) applied a tourniquet.”
GSW right leg “I arrived on scene and observed a male laying on the living room floor holding a towel to his right
upper thigh. There was a belt being used as improvised tourniquet. I had to remove the belt to apply my
tourniquet.”
Stabbing left arm laceration “I observed a male laying on the ground with a piece of clothing wrapped around his left bicep area.
I then applied a tourniquet to his arm.”
Self-inflicted left arm laceration “Upon entering the bedroom a female was laying on the wood floor, surrounded by blood. I noticed a
white towel wrapped around (****) left wrist. (****) was disoriented and began to lose consciousness.
(****) told me she cut her wrist, but didn’t know where the knife ended up. I applied direct pressure to
the towel over the wound, while Officer (****) applied a tourniquet to her left arm. Upon the application
of the tourniquet, I checked for a pulse on her left forearm, and could not feel one, indicating the proper
application of the tourniquet.”
GSW right leg “I ran up to the vehicle and tended to the male, who appeared to have been shot once or twice. One
gunshot wound was in the upper right thigh and the other was through his scrotum. I quickly applied
a tourniquet to the right upper thigh and had another Officer advised dispatch to note a time for my
tourniquet application.”
Self-inflicted right wrist “The female on the ground had a deep laceration to her right wrist with blood actively coming from the
laceration wound. I removed my tourniquet and another officer applied the tourniquet to the female’s right bicep.”
MVA = motor vehicle accident; GSW = gunshot wound; MCA = motorcycle accident; MTA = mass transit accident.
TABLE 5 Response Time for Police and EMS TABLE 6 THREAT Acronym From the Hartford Consensus Group
Response Time (minutes) Median 1. Threat suppression
(mean ± SD) (minutes) 2. Hemorrhage control
Police 6.16 ± 5.16 5 p < .001 3. Rapid Extraction to safety
EMS 10.19 ± 6.82 8 4. Assessment by medical providers
5. Transport to definitive care
FIGURE 1 Response time (minutes) for police versus EMS.
proximity geographically and time-wise to trauma centers, the
liberal use of tourniquets should not result in any complica-
tions since formal medical evaluation will occur within a very
short period of time.
Limitations and Lessons Learned
This study was a retrospective study using an electronic search
for the word “tourniquet,” either in the officers’ computerized
documentation or the records of the communications center. As
such, it is possible that some tourniquet applications were not
recognized or included. In addition, by searching for the word
“tourniquet,” it is likely that patients who might have benefit-
ted from one but did not have one applied were not identified.
Hospital records and follow-up were not available to deter-
mine whether or not an arterial or major venous injury was
present, necessitating the use of the tourniquet. Ideally, direct
feedback from receiving hospitals would be provided as to the
appropriateness of the tourniquet placement and final injury
diagnosed and outcome. This limitation also compromises the
hemorrhage. Application of a tourniquet prior to the onset ability to determine if the bleeding could have been controlled
of hemorrhagic shock has been shown to markedly improved using other methods such as direct pressure or wound packing
mortality compared to placement after shock has developed with gauze or a hemostatic product. Having said that however,
(10% versus 90% respectively). 17,18 several of the criteria for tourniquet application in the field are
subjective in nature and do not require definitive identification
While there were a few cases in which the use of the tourni- of an arterial or venous hemorrhage (Table 2).
quet can be questioned (gunshot wound Achilles area, finger
amputation, one case where the officer documented applica- Consideration should be given to the implementation of for-
tion of the CAT below the wound site, and two cases with mal medical direction and a rigorous quality review and im-
missing information about the rationale for tourniquet use), provement program as it relates to hemorrhage control in the
the majority of applications were consistent with the suggested police department. Since many police departments have im-
criteria for tourniquet placement from the Stop The Bleed ed- plemented body worn cameras, one method of reviewing inci-
ucational program, the military and civilian TCC courses, dents in which tourniquets were applied or other hemorrhage
and the recommendations from the TCC-LEFR course. In control interventions performed would be to review footage
addition, given the urban nature of the city involved and the from every case.
Police Application of Tourniquets | 75