
Page 112 - JSOM Summer 2019
P. 112
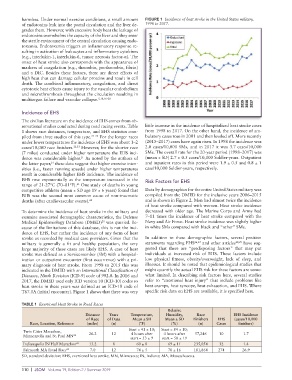
harmless. Under normal exercise conditions, a small amount FIGURE 1 Incidence of heat stroke in the United States military,
of endotoxins leak into the portal circulation and the liver de- 1998 to 2017.
grades them. However, with excessive body heat the leakage of
endotoxins overwhelms the capacity of the liver and they enter
the sterile environment of the central circulation causing endo-
toxemia. Endotoxemia triggers an inflammatory response re-
sulting in activation of leukocytes and inflammatory cytokines
(e.g., interlukin-1, interlukin-6, tumor necrosis factor-α). The
onset of heat stroke also corresponds with the appearance of
markers of coagulation (e.g., thrombin, prothrombin, fibrin)
and a DIC. Besides these factors, there are direct effects of
high heat that can damage cellular proteins and result in cell
death. The combined inflammatory, coagulation, and direct
cytotoxic heat effects cause injury to the vascular endothelium
and microthrombosis throughout the circulation resulting in
multiorgan failure and vascular collapse. 5,10,16–20
Incidence of EHS
The civilian literature on the incidence of EHS comes from ob-
servational studies conducted during road racing events. Table little increase in the incidence of hospitalized heat stroke cases
1 shows race distances, temperature, and EHS statistics com- from 1998 to 2017. On the other hand, the incidence of am-
piled from three studies of this type. 21–23 For the longer races bulatory cases rose in 2001 and then leveled off. More recently
under lower temperatures the incidence of EHS was about 1–2 (2015–2017) cases have again risen. In 1998 the incidence was
cases/10,000 race finishers. 22,23 However, for the shorter race 2.0 cases/10,000 SMs, and in 2017 it was 3.7 cases/10,000
(7 miles) conducted under higher temperature the EHS inci- SMs. The overall rate for the 20-year period (1998–2017) was
dence was considerable higher. As noted by the authors of (mean ± SD) 2.7 ± 0.5 cases/10,000 Soldier-years. Outpatient
21
the latter paper, these data suggest that higher exercise inten- and inpatient rates in this period were 1.9 ± 0.5 and 0.8 ± 1
21
sities (i.e., faster running speeds) under higher temperatures case/10,000 Soldier-years, respectively.
result in considerable higher EHS incidence. The incidence of
EHS rose exponentially as the temperature increased in the Risk Factors for EHS
range of 21-27°C (70–81°F). One study of deaths in young
21
competitive athletes (mean ± SD age 19 ± 6 years) found that Data by demographics for the entire United States military was
EHS was the second most common cause of non-traumatic compiled from the DMED for the inclusive years 2006–2015
deaths (after cardiovascular events). 24 and is shown in Figure 2. Men had almost twice the incidence
of heat stroke compared with women. Heat stroke incidence
To determine the incidence of heat stroke in the military and decreased with older age. The Marine Corps and Army had
examine associated demographic characteristics, the Defense 7–11 times the incidence of heat stroke compared with the
Medical Epidemiology Database (DMED) was queried. Be- Navy and Air Force. Heat stroke incidence was slightly higher
25
cause of the limitations of this database, this is not the inci- in white SMs compared with black and “other” SMs.
dence of EHS, but rather the incidence of any form of heat
stroke as recorded by medical care providers. Given that the In addition to these demographic factors, several position
military is generally a fit and healthy population, the very statements regarding EHS 26,27 and other articles 28,29 have sug-
large majority of these cases are likely EHS. A case of heat gested that there are “predisposing factors” that may put
stroke was defined as a Servicemember (SM) with a hospital- individuals at increased risk of EHS. These factors include
ization or outpatient encounter (first occurrence) with a pri- low physical fitness, obesity/overweight, lack of sleep, and
mary diagnosis of heat stroke. From 1998 to 2015 this was illnesses. It should be noted that epidemiological studies that
indicated in the DMED with an International Classification of might quantify the actual EHS risk for these factors are some-
Diseases, Ninth Revision (ICD-9) code of 992.0. In 2016 and what limited. In describing risk factors here, several studies
2017, the DMED used only ICD version 10 (ICD-10) codes so refer to “exertional heat injury” that include problems like
heat stroke in these years was defined as an ICD-10 code of heat cramps, heat syncope, heat exhaustion, and EHS. Where
T67.0A (initial encounter). Figure 1 shows that there was very specific risk data on EHS are available, it is specified here.
TABLE 1 Exertional Heat Stroke in Road Races
Relative
Distance Years Temperature, Humidity, Race EHS Incidence
of Race of Data Mean ± SD Mean ± SD Finishers EHS (cases/10,000
Race, Location, Reference (miles) (n) (°F) (%) (n) Cases finishers)
Start = 41 ± 10; Start = 84 ± 10;
Twin Cities Marathon,
Minneapolis and St. Paul MN 23 26.2 12 4 hours after 4 hours after 57,246 10 1.7
start = 53 ± 9 start = 58 ± 19
Indianapolis IN Half Marathon 22 13.2 8 60 ± 8 69 ± 11 235,054 32 1.4
Falmouth MA Road Race 21 7.0 12 74 ± 5 70 ± 16 101,864 274 26.9
SD, standard deviation; EHS, exertional heat stroke; MN, Minnesota; IN, Indiana; MA, Massachusetts.
110 | JSOM Volume 19, Edition 2 / Summer 2019