
Page 80 - JSOM Winter 2018
P. 80
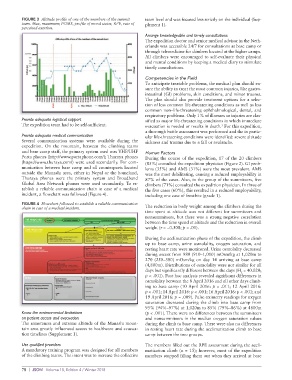
FIGURE 3 Altitude profile of one of the members of the summit team level and was focused less strictly on the individual (Sup-
team. Max, maximum; POMS, profile of mood states; RPE, rate of plement 1).
perceived exertion.
Arrange knowledgeable and timely consultations
The expedition doctor and senior medical advisor in the Neth-
erlands was accessible 24/7 for consultations at base camp or
through telemedicine for climbers located at the higher camps.
All climbers were encouraged to self-evaluate their physical
and mental conditions by keeping a medical diary to stimulate
timely consultations.
Competencies in the Field
To anticipate treatable problems, the medical plan should en-
sure the ability to treat the most common injuries, like gastro-
intestinal (GI) problems, skin conditions, and minor trauma.
The plan should also provide treatment options for a selec-
tion of less common life-threatening conditions as well as less
common non–life-threatening ophthalmological, dental, and
respiratory problems. Only 1% of illnesses or injuries are clas-
Provide adequate logistical support sified as major life-threatening conditions in which immediate
The expedition team had to be self-sufficient. evacuation is needed or results in death. For this expedition,
3
a thorough battle assessment was performed and the in partic-
Provide adequate medical communication ular life-threatening conditions were identified: severe altitude
Several communication systems were available during the sickness and trauma due to a fall or avalanche.
expedition. On the mountain, between the climbing teams
and base camp staff, the primary system used was VHF/UHF Human Factors
Porta phones (http://www.portaphone.com/); Thuraya phones During the course of the expedition, 17 of the 20 climbers
(https://www.thuraya.com/) were used secondarily. For com- (85%) consulted the expedition physician (Figure 2). GI prob-
munication between base camp and all counterparts located lems (35%) and AMS (31%) were the most prevalent. AMS
outside the Manaslu area, either in Nepal or the homeland, was the most debilitating, causing a reduced employability in
Thuraya phones were the primary system and Broadband 87% of the cases. Also, in the group of the summiteers, five
Global Area Network phones were used secondarily. To es- climbers (71%) consulted the expedition physician. In three of
tablish a reliable communication chain in case of a medical the five cases (60%), this resulted in a reduced employability,
incident, a flowchart was followed (Figure 4). including one case of frostbite (grade 1).
FIGURE 4 Flowchart followed to establish a reliable communication The reduction in body weight among the climbers during the
chain in case of a medical incident.
time spent at altitude was not different for summiteers and
nonsummiteers, but there was a strong negative correlation
between the time spend at altitude and the reduction in overall
weight (r = −0.508; p < .01).
During the acclimatization phase of the expedition, the climb
up to base camp, urine osmolality, oxygen saturation, and
resting heart rate were monitored. Urine osmolality decreased
during ascent from 980 (910–1,010) mOsm/kg at 1,020m to
270 (250–380) mOsm/kg on day 14 arriving at base camp
(4,800m). Distributions of osmolality were not similar for all
days but significantly different between the days (H = 40.020;
5
p < .001). Post hoc analysis revealed significant differences in
osmolality between the 8 April 2016 and all other days climb-
ing to base camp (10 April 2016: p = .011; 12 April 2016:
p < .001; 14 April 2016: p < .001; 16 April 2016: p < .001; and
19 April 2016: p = .009). Pulse oximetry readings for oxygen
saturation decreased during the climb into base camp from
95% (94%–97%) at 1,020m to 85% (79%–86%) at 4800m
Know the environmental limitations (p < .001). There were no differences between the summiteers
on patient access and evacuation and nonsummiteers in the median oxygen saturation values
The remoteness and extreme altitude of the Manaslu moun- during the climb to base camp. There were also no differences
tain area greatly influenced access to healthcare and evacua- in resting heart rate during the acclimatization climb to base
tion timelines (Supplement 1). camp between the two groups.
Use qualified providers The members filled out the RPE assessment during the accli-
A mandatory training program was designed for all members matization climb (n = 15); however, most of the expedition
of the climbing teams. The intent was to increase the collective members stopped filling them out when they arrived at base
78 | JSOM Volume 18, Edition 4 / Winter 2018