
Page 37 - JSOM Fall 2018
P. 37
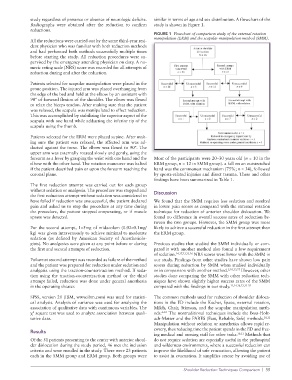
study regardless of presence or absence of neurologic deficits. similar in terms of age and sex distribution. A flowchart of the
Radiographs were obtained after the reduction to confirm study is shown in Figure 1.
reductions.
FIGURE 1 Flowchart of comparison study of the external rotation
manipulation (ERM) and the scapular manipulation method (SMM).
All the reductions were carried out by the same thirdyear resi
dent physician who was familiar with both reduction methods
and had performed both methods successfully multiple times
before starting the study. All reduction procedures were su
pervised by the emergency attending physician on duty. A nu
meric rating scale (NRS) score was recorded for all attempts of
reduction during and after the reduction.
Patients selected for scapular manipulation were placed in the
prone position. The injured arm was placed overhanging from
the edge of the bed and held at the elbow by an assistant with
90° of forward flexion of the shoulder. The elbow was flexed
to relax the biceps tendon. After making sure that the patient
was relaxed, the scapula was manipulated to effect reduction.
This was accomplished by stabilizing the superior aspect of the
scapula with one hand while adducting the inferior tip of the
scapula using the thumb.
Patients selected for the ERM were placed supine. After mak
ing sure the patient was relaxed, the affected arm was ad
ducted against the torso. The elbow was flexed to 90°. The
upper arm was externally rotated slowly and gently, using the
forearm as a lever by grasping the wrist with one hand and the Most of the participants were 20–30 years old (n = 10 in the
elbow with the other hand. The rotation maneuver was halted ERM group, n = 12 in SMM group). a fall on an outstretched
if the patient described pain or upon the forearm reaching the hand was the commonest mechanism (75%; n = 34), followed
coronal plane. by sportsrelated injuries and direct trauma. These and other
findings have been summarized in Table 1.
The first reduction attempt was carried out for each group
without sedation or analgesia. The procedure was stopped and discussion
the first reduction attempt without sedation was considered to
have failed if reduction was unsuccessful, the patient declared We found that the SMM requires less sedation and resulted
pain and asked us to stop the procedure at any time during in lower pain scores as compared with the external rotation
the procedure, the patient stopped cooperating, or if muscle technique for reduction of anterior shoulder dislocation. We
spasm was detected. found no difference in overall success rates of reduction be
tween the two groups. However, the SMM group was more
For the second attempt, 1–5mg of midazolam (0.02–0.1mg/ likely to achieve a successful reduction in the first attempt than
kg) was given intravenously to achieve minimal to moderate the ERM group.
sedation (as defined by American Society of Anesthesiolo
gists). No analgesics were given at any point before or during Previous studies that studied the SMM individually or com
the first and second attempts of reduction. pared it with another method also found a low requirement
of sedation. 14,17,23,25,26 NRS scores were lower with the SMM in
Failure at second attempt was recorded as failure of the method our study. Findings from other studies have shown low pain
and the patient was prepared for reduction under sedation and scores during reduction by SMM when studied individually
analgesia using the tractioncountertraction method. If seda or in comparison with another method. 5,10,23,27 However, other
tion using the tractioncountertraction method or the third studies done comparing the SMM with other reduction tech
attempt failed, reduction was done under general anesthesia niques have shown slightly higher success rates of the SMM
in the operating theater. compared with the findings in our study. 12,14,16,23,2529
SPSS, version 20 (IBM, www.ibm.com) was used for statisti The common methods used for reduction of shoulder disloca
cal analysis. Analysis of variance was used for analyzing the tions in the ED include the Kocher, Spaso, external rotation,
association of qualitative data with continuous variables. The Milch, Chair, Stimson, and the scapular manipulation meth
χ square test was used to analyze association between quali ods. 4–10 The nontraditional techniques include the BossHolz
2
tative data. achMatter and the FARES (Fast, Reliable, Safe) methods. 10,11
Manipulation without sedation or anesthetics allows rapid re
covery, thus reducing time the patient spends in the ED and free
results
ing medical and nursing staff for other tasks. 30,31 Methods that
Of the 51 patients presenting to the center with anterior shoul do not require sedation are especially useful in the prehospital
der dislocation during the study period, 46 met the inclusion and wilderness environments, where a successful reduction can
criteria and were enrolled in the study. There were 23 patients improve the likelihood of safe evacuation, allowing the patient
each in the SMM group and ERM group. Both groups were to assist in evacuation. It simplifies rescue by avoiding use of
Shoulder Reduction Techniques Comparison | 35