
Page 85 - JSOM Summer 2018
P. 85
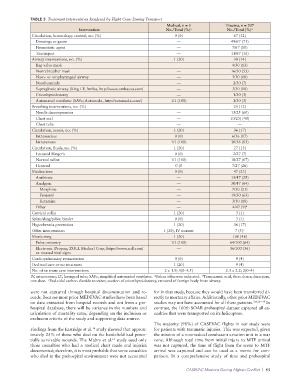
TABLE 3 Treatment Interventions Rendered by Flight Crew During Transport
Medical, n = 5 Trauma, n = 207
Intervention No./Total (%) a No./Total (%) a
Circulation, hemorrhage control, no. (%) 0 (0) 67 (32)
Dressings or gauze — 49/67 (73)
Hemostatic agent — 7/67 (10)
Tourniquet — 11/67 (16)
Airway interventions, no. (%) 1 (20) 30 (14)
Bag-valve-mask 4/30 (13)
Nonrebreather mask — 16/30 (53)
Naso- or oropharyngeal airway — 3/30 (10)
Nasal cannula — 2/30 (7)
Supraglottic airway (King LT; Ambu, http://www.ambuusa.com) — 3/30 (10)
Cricothyroidotomy — 1/30 (3)
Automated ventilator (SAVe; Automedx, http://automedx.com/) 1/1 (100) 1/30 (3)
Breathing interventions, no. (%) 25 (12)
Needle decompression — 15/25 (60)
Chest seal — 10/25) (40)
Chest tube — —
Circulation, access, no. (%) 1 (20) 36 (17)
Intraosseous 0 (0) 6/36 (17)
Intravenous 1/1 (100) 30/36 (83)
Circulation, fluids, no. (%) 1 (20) 27 (13)
Lactated Ringer’s 0 (0) 2/27 (7)
Normal saline 1/1 (100) 18/27 (67)
Hextend 0 (0 7/27 (26)
Medications 0 (0) 47 (23)
Antibiotic — 13/47 (28)
Analgesic — 30/47 (64)
Morphine — 7/30 (23)
Fentanyl — 19/30 (63)
Ketamine — 3/30 (10)
Other — 4/47 (9) b
Cervical collar 1 (20) 3 (1)
Splint/sling/pelvic binder 0 (0) 3 (1)
Hypothermia prevention 1 (20) 36 (17)
Other interventions 1 (20), IV warmer 7 (3) c
Monitoring 1 (20) 100 (48)
Pulse oximetry 1/1 (100) 64/100 (64)
Electronic (Propaq; ZOLL Medical Corp, https://www.zoll.com) — 36/100 (36)
or manual vital signs
Cardiopulmonary resuscitation 0 (0) 9 (4)
Declined care or no treatment 1 (20) 9 (4)
No. of en route care interventions 2 ± 1.9; 3(0–3.5) 2.3 ± 2.2; 2(0–4)
IV, intravenous; LT, laryngeal tube; SAVe, simplified automated ventilator. Unless otherwise indicated. Tranexamic acid, three doses; diazepam,
b
a
c
one dose. End-tidal carbon dioxide monitor, suction of cricothyroidotomy, removal of foreign body from airway.
were not captured through hospital documentation and re- for in that study, because they would have been transferred di-
cords. Because most prior MEDEVAC studies have been based rectly to mortuary affairs. Additionally, other prior MEDEVAC
on data extracted from hospital records and not from a pre- studies may not have accounted for all these patients. 3,4,16-–19 In
hospital database, there will be variance in the numbers and contrast, the 160th SOAR prehospital dataset captured all ca-
calculation of mortality rates, depending on the inclusion or sualties that were transported on its helicopters.
exclusion criteria of the study and supporting data source.
The majority (98%) of CASEVAC flights in our study were
14
Findings from the Eastridge et al. study showed that approx- for patients with traumatic injuries. This was expected, given
imately 25% of those who died on the battlefield had poten- the mission of a nonmedical combatant aviation unit in a war
tially survivable wounds. The Mabry et al. study used only zone. Although total time from initial injury to MTF arrival
15
those casualties who had a medical chart made and injuries was not captured, the time of flight from the scene to MTF
documented; therefore, it is most probable that some casualties arrival was captured and can be used as a metric for com-
who died in the prehospital environment were not accounted parison. In a comprehensive study of time and prehospital
CASEVAC Missions During Afghan Conflict | 83