
Page 84 - JSOM Summer 2018
P. 84
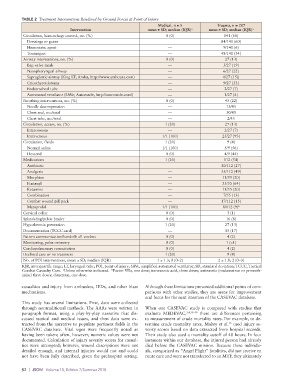
TABLE 2 Treatment Interventions Rendered by Ground Forces at Point of Injury
Medical, n = 5 Trauma, n = 207
Intervention mean ± SD; median (IQR) a mean ± SD; median (IQR) a
Circulation, hemorrhage control, no. (%) 0 (0) 141 (68)
Dressings or gauze 84/141 (60)
Hemostatic agent — 9/141 (6)
Tourniquet — 48/141 (34)
Airway interventions, no. (%) 0 (0) 27 (13)
Bag-valve-mask — 5/27 (19)
Nasopharyngeal airway — 6/27 (22)
Supraglottic airway (King LT; Ambu, http://www.ambuusa.com) — 4/27 (15))
Cricothyroidotomy — 9/27 (33)
Endotracheal tube — 2/27 (7)
Automated ventilator (SAVe; Automedx, http://automedx.com/) — 1/27 (4)
Breathing interventions, no. (%) 0 (0) 45 (22)
Needle decompression — 13/45
Chest seal, no./total — 30/45
Chest tube, no./total — 2/45
Circulation, access, no. (%) 1 (20) 27 (13)
Intraosseous — 2/27 (7)
Intravenous 1/1 (100) 25/27 (93)
Circulation, fluids 1 (20) 9 (4)
Normal saline 1/1 (100) 5/9 (56)
Hextend 0 (0) 4/9 (44)
Medications 1 (20) 112 (54)
Antibiotic 30/112 (27)
Analgesic — 55/112 (49)
Morphine — 11/55 (20)
Fentanyl — 35/55 (64)
Ketamine — 11/55 (20)
Combination — 7/55 (13)
Combat wound pill pack — 17/112 (15)
Metoprolol 1/1 (100) 8/112 (9) b
Cervical collar 0 (0) 3 (1)
Splint/sling/pelvic binder 0 (0) 16 (8)
Hypothermia prevention 1 (20) 27 (13)
Documentation (TCCC card) — 35 (17)
Patient communication/handoff: all voxbox 0 (0) 4 (2)
Monitoring, pulse oximetry 0 (0) 1 (<1)
Cardiopulmonary resuscitation 0 (0) 4 (2)
Declined care or no treatment 1 (20) 9 (4)
No. of POI interventions, mean ± SD; median (IQR) 1 ± 1.3; 0 (0–2) 2 ± 1.8; 2 (0–3)
IQR, interquartile range; LT, laryngeal tube; POI, point of injury; SAVe, simplified automated ventilator; SD, standard deviation; TCCC, Tactical
Combat Casualty Care. Unless otherwise indicated. Factor VIIa, one dose; tranexamic acid, three doses; antiemetic (ondansetron or prometh-
a
b
azine) three doses; diazepam, one dose.
casualties and injury from ambushes, IEDs, and other blast Although these limitations prevented additional points of com-
mechanisms. parisons with other studies, they are areas for improvement
and focus for the next iteration of the CASEVAC database.
This study has several limitations. First, data were collected
through nontraditional methods. The AARs were written in When our CASEVAC study is compared with studies that
paragraph format, using a play-by-play narrative that dis- evaluate MEDEVAC, 3,4,15–19 there are differences pertaining
cussed tactical and medical issues, and then data were ex- to measurement of crude mortality rates. For example, to de-
15
tracted from the narrative to populate pertinent fields in the termine crude mortality rates, Mabry et al. used injury se-
CASEVAC database. Vital signs were frequently noted as verity scores based on data extracted from hospital records.
having been taken; often, however, numeric values were not Their study also used a mortality cutoff of 48 hours. In four
documented. Calculation of injury severity scores for casual- instances within our database, the injured person had already
ties were attempted; however, wound descriptions were not died before the CASEVAC mission. Because these individu-
detailed enough, and internal injuries would not and could als, categorized as “Angel Flight” fatalities, did not receive en
not have been fully described, given the prehospital setting. route care and were not transferred to an MTF, they ultimately
82 | JSOM Volume 18, Edition 2/Summer 2018