
Page 34 - JSOM Summer 2018
P. 34
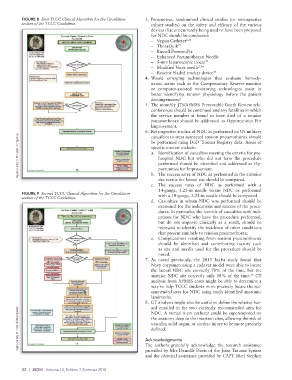
FIGURE 8 First TCCC Clinical Algorithm for the Circulation 3. Prospective, randomized clinical studies (or retrospective
section of the TCCC Guidelines. cohort studies) on the safety and efficacy of the various
devices that are currently being used or have been proposed
for NDC should be conducted:
– Vygon Catheter 6,66
– ThoraQuik 73
– Russell PneumoFix
– Enhanced Pneumothorax Needle
– 5-mm laparoscopic trocar 72
– Modified Veres needle 7,74
– Reactor bladed trochar device 75
4. Would emerging technologies that evaluate hemody-
namic status such as the Compensatory Reserve monitor
or computer-assisted monitoring technologies assist in
better identifying tension physiology before the patient
decompensates?
5. The monthly JTS/AFMES Preventable Death Review tele-
conferences should be continued and any fatalities in which
the service member is found to have died of a tension
pneumothorax should be addressed as Opportunities For
Improvement.
6. Retrospective studies of NDC as performed on US military
Figure courtesy of Mr Harold Montgomery. specific interest include:
casualties to treat suspected tension pneumothorax should
be performed using DoD Trauma Registry data. Areas of
a. Identification of casualties meeting the criteria for pre-
hospital NDC but who did not have the procedure
performed should be identified and addressed as Op-
portunities for Improvement.
b. The success rates of NDC as performed in the anterior
site versus the lateral site should be compared.
c. The success rates of NDC as performed with a
14-gauge, 3.25-in needle versus NDC as performed
FIGURE 9 Second TCCC Clinical Algorithm for the Circulation with a 10-gauge, 3.25-in needle should be compared.
section of the TCCC Guidelines.
d. Casualties in whom NDC was performed should be
examined for the indications and success of the proce-
dures. In particular, the records of casualties with indi-
cations for NDC who have the procedure performed,
but do not improve clinically as a result, should be
reviewed to identify the incidence of other conditions
that present similarly to tension pneumothorax.
e. Complications resulting from tension pneumothorax
should be identified and contributing factors such
as site and needle used for the procedure should be
noted.
7. As noted previously, the 2015 Inaba study found that
Navy corpsmen using a cadaver model were able to locate
the lateral NDC site correctly 78% of the time, but the
anterior NDC site correctly only 18% of the time. CT
15
analysis from AFMES cases might be able to determine a
way to help TCCC students more precisely locate the rec-
ommended sites for NDC using easily identified anatomic
landmarks.
8. CT analysis might also be useful to define the relative haz-
ard entailed in the two currently recommended sites for
Figure courtesy of Mr Harold Montgomery. Acknowledgments
NDC. A virtual 8-cm catheter could be superimposed on
the anatomy deep to the insertion sites, allowing the risk of
vascular, solid organ, or cardiac injury to be more precisely
defined.
The authors gratefully acknowledge the research assistance
provided by Mrs Danielle Davis of the Joint Trauma System
and the editorial assistance provided by CAPT (Ret) Stephen
32 | JSOM Volume 18, Edition 2/Summer 2018