
Page 33 - JSOM Summer 2018
P. 33
2. Initial treatment of suspected tension pneumothorax: e. If a casualty in shock is not responding to fluid resus-
– If the casualty has a chest seal in place, burp or re- citation, consider untreated tension pneumothorax as
move the chest seal. a possible cause of refractory shock. Thoracic trauma,
– Establish pulse oximetry monitoring. persistent respiratory distress, absent breath sounds,
– Place the casualty in the supine or recovery position and hemoglobin oxygen saturation < 90% support
unless he or she is conscious and needs to sit up to this diagnosis. Treat as indicated with repeated NDC
help keep the airway clear as a result of maxillofacial or finger thoracostomy/chest tube insertion at the fifth
trauma. ICS in the AAL, according to the skills, experience, and
– Decompress the chest on the side of the injury with authorizations of the treating medical provider. Note
a 14-gauge or a 10-gauge, 3.25 inch needle/catheter that if finger thoracostomy is used, it may not remain
unit. patent and finger decompression through the incision
– If a casualty has significant torso trauma or primary may have to be repeated. Consider decompressing the
blast injury and is in traumatic cardiac arrest (no opposite side of the chest if indicated based on the
pulse, no respirations, no response to painful stimuli, mechanism of injury and physical findings.
no other signs of life), decompress both sides of the
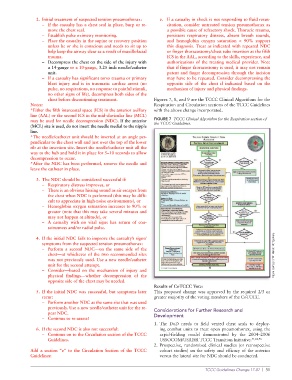
chest before discontinuing treatment. Figures 7, 8, and 9 are the TCCC Clinical Algorithms for the
Notes: Respiration and Circulation sections of the TCCC Guidelines
*Either the fifth intercostal space (ICS) in the anterior axillary with the above change incorporated.
line (AAL) or the second ICS in the mid-clavicular line (MCL)
may be used for needle decompression (NDC). If the anterior FIGURE 7 TCCC Clinical Algorithm for the Respiration section of
(MCL) site is used, do not insert the needle medial to the nipple the TCCC Guidelines.
line.
*The needle/catheter unit should be inserted at an angle per-
pendicular to the chest wall and just over the top of the lower
rib at the insertion site. Insert the needle/catheter unit all the
way to the hub and hold it in place for 5–10 seconds to allow
decompression to occur.
*After the NDC has been performed, remove the needle and
leave the catheter in place.
3. The NDC should be considered successful if:
– Respiratory distress improves, or
– There is an obvious hissing sound as air escapes from
the chest when NDC is performed (this may be diffi-
cult to appreciate in high-noise environments), or
– Hemoglobin oxygen saturation increases to 90% or
greater (note that this may take several minutes and
may not happen at altitude), or
– A casualty with no vital signs has return of con-
sciousness and/or radial pulse.
4. If the initial NDC fails to improve the casualty’s signs/
symptoms from the suspected tension pneumothorax:
– Perform a second NDC—on the same side of the
chest—at whichever of the two recommended sites Figure courtesy of Mr Harold Montgomery.
was not previously used. Use a new needle/catheter
unit for the second attempt.
– Consider—based on the mechanism of injury and
physical findings—whether decompression of the
opposite side of the chest may be needed.
Results of CoTCCC Vote:
5. If the initial NDC was successful, but symptoms later This proposed change was approved by the required 2/3 or
recur: greater majority of the voting members of the CoTCCC.
– Perform another NDC at the same site that was used
previously. Use a new needle/catheter unit for the re- Considerations for Further Research and
peat NDC. Development
– Continue to re-assess!
1. The DoD needs to field vented chest seals to deploy-
6. If the second NDC is also not successful: ing combat units to treat open pneumothorax, using the
– Continue on to the Circulation section of the TCCC rapid-fielding model demonstrated by the 2004–2006
Guidelines. USSOCOM/USAISR TCCC Transition Initiative. 51,62,96
2. Prospective, randomized clinical studies (or retrospective
Add a section “e” to the Circulation Section of the TCCC cohort studies) on the safety and efficacy of the anterior
Guidelines: versus the lateral site for NDC should be conducted.
TCCC Guidelines Change 17-02 | 31 | 31
TCCC Guidelines Change 17-02