
Page 148 - Journal of Special Operations Medicine - Spring 2017
P. 148
included four cases with acute gastroenteritis, one with Table 4 Infil/Exfil Modes, Disposition, Duration and
meningitis, one with dengue fever, one with Lyme dis- Mortality
ease, and one with flu-like illness and rash. The cardiac No. (%)
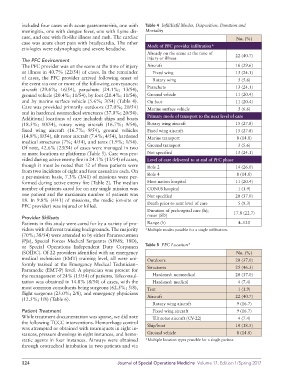
case was acute chest pain with bradycardia. The other Mode of PFC provider infiltration*
etiologies were odynophagia and severe headache.
Already on the scene at the time of 22 (40.7)
The PFC Environment injury or illness
The PFC provider was on the scene at the time of injury Aircraft 16 (29.6)
or illness in 40.7% (22/54) of cases. In the remainder Fixed wing 13 (24.1)
of cases, the PFC provider arrived following onset of Rotary wing 3 (5.6)
the event via one or more of the following conveyances:
aircraft (29.6%; 16/54), parachute (24.1%; 13/54), Parachute 13 (24.1)
ground vehicle (20.4%; 11/54), by foot (20.4%; 11/54), Ground vehicle 11 (20.4)
and by marine surface vehicle (5.6%; 3/54) (Table 4). On foot 11 (20.4)
Care was provided primarily outdoors (37.0%; 20/54) Marine surface vehicle 3 (6.6)
and in hardened nonmedical structures (37.0%; 20/54).
Additional locations of care included: ships and boats Primary mode of transport to the next level of care
(18.5%; 10/54), rotary wing aircraft (16.7%; 9/54), Rotary wing aircraft 15 (27.8)
fixed wing aircraft (16.7%; 9/54), ground vehicles Fixed wing aircraft 15 (27.8)
(14.8%; 8/54), tilt rotor aircraft (7.4%; 4/54), hardened Marine transport 8 (14.8)
medical structures (7%; 4/54), and tents (1.9%; 1/54).
Of note, 42.6% (23/54) of cases were managed in two Ground transport 3 (5.6)
or more locations or platforms (Table 5). Care was pro- Not specified 13 (24.1)
vided during active enemy fire in 24.1% (13/54) of cases, Level of care delivered to at end of PFC phase
though it must be noted that 12 of these patients were Role 2 14 (26.0)
from two incidents of eight and four casualties each. On Role 4 8 (14.8)
a per-mission basis, 7.3% (3/41) of missions were per-
formed during active enemy fire (Table 2). The median Host nation hospital 11 (20.4)
number of patients cared for on any single mission was CONUS hospital 1 (1.9)
one patient and the maximum number of patients was Not specified 20 (37.0)
18. In 9.8% (4/41) of missions, the medic (on-site or Death prior to next level of care 5 (9.3)
PFC provider) was injured or killed.
Duration of prehospital care (h); 17.8 (22.7)
Provider Skillsets mean (SD)
Patients in this study were cared for by a variety of pro- Range (h) 4–120
viders with different training backgrounds. The majority *Multiple modes possible for a single infiltration.
(70%; 38/54) were attended to by either Pararescuemen
(PJs), Special Forces Medical Sergeants (SFMS; 18D),
or Special Operations Independent Duty Corpsmen Table 5 PFC Location*
(SOIDC). Of 22 providers identified with an emergency No. (%)
medical technician (EMT) training level, all were uni- Outdoors 20 (37.0)
formly trained at the Emergency Medical Technician– Structures 25 (46.3)
Paramedic (EMT-P) level. A physician was present for
the management of 24% (15/54) of patients. Teleconsul- Hardened: nonmedical 20 (37.0)
tation was obtained in 14.8% (8/54) of cases, with the Hardened: medical 4 (7.4)
most common consultants being surgeons (62.5%; 5/8), Tent 1 (1.9)
flight surgeons (25.0%; 2/8), and emergency physicians Aircraft 22 (40.7)
(12.5%; 1/8) (Table 6).
Rotary wing aircraft 9 (16.7)
Patient Treatment Fixed wing aircraft 9 (16.7)
While treatment documentation was sparse, we did note Tilt rotor aircraft (CV-22) 4 (7.4)
the following TCCC interventions. Hemorrhage control Ship/boat 10 (18.5)
was attempted or obtained with tourniquets in eight in-
stances, pressure dressings in eight instances, and hemo- Ground vehicle 8 (14.8)
static agents in four instances. Airways were obtained *Multiple location types possible for a single patient.
through orotracheal intubation in two patients and via
124 Journal of Special Operations Medicine Volume 17, Edition 1/Spring 2017