
Page 144 - Journal of Special Operations Medicine - Spring 2017
P. 144
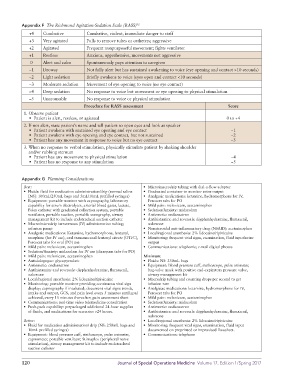
Appendix F The Richmond Agitation-Sedation Scale (RASS) 12
+4 Combative Combative, violent, immediate danger to staff
+3 Very agitated Pulls to remove tubes or catheters; aggressive
+2 Agitated Frequent nonpurposeful movement; fights ventilator
+1 Restless Anxious, apprehensive, movements not aggressive
0 Alert and calm Spontaneously pays attention to caregiver
−1 Drowsy Not fully alert but has sustained awakening to voice (eye opening and contact >10 seconds)
−2 Light sedation Briefly awakens to voice (eyes open and contact <10 seconds)
−3 Moderate sedation Movement of eye opening to voice (no eye contact)
−4 Deep sedation No response to voice but movement or eye opening to physical stimulation
−5 Unarousable No response to voice or physical stimulation
Procedure for RASS assessment Score
1. Observe patient
• Patient is alert, restless, or agitated 0 to +4
2. If not alert, state patient’s name and tell patient to open eyes and look at speaker
• Patient awakens with sustained eye opening and eye contact −1
• Patient awakens with eye opening and eye contact, but not sustained −2
• Patient has any movement in response to voice but no eye contact –3
3. When no response to verbal stimulation, physically stimulate patient by shaking shoulder
and/or rubbing sternum
• Patient has any movement to physical stimulation −4
• Patient has no response to any stimulation −5
Appendix G Planning Considerations
Best: • Micro/macrodrip tubing with dial-a-flow adaptor
• Fluids: fluid for medication administration/drip (normal saline • Graduated container to monitor urine output
[NS]: 100mL/250mL bags and 5mL/10mL prefilled syringes) • Analgesic medications: ketamine, hydromorphone for IV,
• Equipment: portable monitor with capnography, laboratory Percocet tabs for PO
capability for serum electrolytes, arterial blood gases, lactate, • Mild pain: meloxicam, acetaminophen
Foley catheter with graduated collection system, portable • Sedation/Anxiety: midazolam
ventilator, portable suction, portable sonography, airway • Antiemetic: ondansatron
management kit to include endotracheal suction catheter • Antihistamine and reversals: diyphenhydramine, flumazenil,
• Macro/microdrip intravenous (IV) administration tubing; naloxone
infusion pump • Nonsteroidal anti-inflammatory drug (NSAID): acetminophen
• Analgesic medications: Ketamine, hydromorphone, fentanyl, • Local/regional anesthesia: 2% lidocaine/ripivicaine
morphine (for IV use), oral transmucosal fentanyl citrate (OTFC), • Monitoring: frequent vital signs, examination, fluid input/urine
Percocet tabs for oral (PO) use output
• Mild pain: meloxicam, acetaminophen • Communications: telephonic; e-mail digital photos
• Sedation/Anxiety: midazolam for IV use (diazepam tabs for PO)
• Mild pain: meloxicam, acetaminophen Minimum:
• Antisialogogue: glycopyrrolate • Fluids: NS: 250mL bags
• Antiemetic: ondansatron • Equipment: blood pressure cuff, stethoscope, pulse oximeter,
• Antihistamine and reversals: diyphenhydramine, flumazenil, bag-valve mask with positive end-expiratory pressure valve,
naloxone airway management kit
• Local/regional anesthesia: 2% lidocaine/ripivicaine • Macrodrip tubing and counting drops per second to get
• Monitoring: portable monitor providing continuous vital sign infusion rate
display; capnography if intubated; document vital signs trends, • Analgisiac medications: ketamine, hydromorphone for IV,
intake and output, GCS, and pain level every 5 minutes until goal Percocet tabs for PO
achieved, every 15 minutes thereafter; pain assessment sheet • Mild pain: meloxicam, acetaminophen
• Communications: real-time video telemedicine consultation • Sedation/Anxiety: midazolam
• Push-pack capability: prepackaged additional 24-hour supplies • Antiemetic: ondansatron
of fluids, and medications for scenarios >24 hours. • Antihistamine and reversals: diyphenhydramine, flumazenil,
naloxone
Better: • Local/regional anesthesia: 2% lidocaine/ripivicaine
• Fluid for medication administration/ drip (NS: 250mL bags and • Monitoring: frequent vital signs, examination, fluid input
10mL prefilled syringes) documented on preprinted or improvised flowsheet.
• Equipment: blood pressure cuff, stethoscope, pulse oximeter, • Communications: telephone
capnometer, portable ventilator, Stimuplex (peripheral nerve
stimulation), airway management kit to include endotracheal
suction catheter
120 Journal of Special Operations Medicine Volume 17, Edition 1/Spring 2017