
Page 60 - Journal of Special Operations Medicine - Winter 2014
P. 60
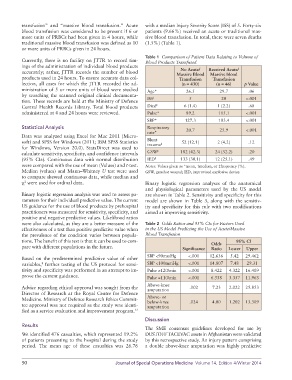
transfusion” and “massive blood transfusion.” Acute with a median Injury Severity Score (ISS) of 5. Forty-six
blood transfusion was considered to be present if 6 or patients (9.66%) received an acute or traditional mas-
more units of PRBCs had been given in 4 hours, while sive blood transfusion. In total, there were seven deaths
traditional massive blood transfusion was defined as 10 (1.5%) (Table 1).
or more units of PRBCs given in 24 hours.
Table 1 Comparison of Patient Data Relating to Volume of
Currently, there is no facility on JTTR to record tim- Blood Products Transfused
ings of the administration of individual blood products No Acute/ Received Acute/
accurately; rather, JTTR records the number of blood Massive Blood Massive blood
products used in 24 hours. To ensure accurate data col- Transfusion Transfusion
lection, all cases for which the JTTR recorded the ad- (n = 430) (n = 46) p Value
ministration of 5 or more units of blood were studied Age* 26.5 29.7 .06
by searching the scanned original clinical documenta- †
tion. These records are held at the Ministry of Defence ISS 5 20 <.001
‡
Central Health Records Library. Total blood products Died 6 (1.4) 1 (2.2) .68
administered at 4 and 24 hours were reviewed. Pulse* 89.2 115.1 <.001
SBP* 127.3 103.4 <.001
Statistical Analysis Respiratory 20.7 25.9 <.001
rate*
Data was analyzed using Excel for Mac 2011 (Micro-
soft) and SPSS for Windows (2011; IBM SPSS Statistics Blunt ‡ 52 (12.1) 2 (4.2) .12
trauma
for Windows, Version 20.0). StatsDirect was used to
calculate sensitivity, specificity, and confidence intervals GSW ‡ 182 (42.3) 24 (52.2) .20
(95% CIs). Continuous data with normal distribution IED ‡ 133 (30.1) 12 (25.1) .49
were compared with the use of mean (Values) and t-test. Notes: Values given as *mean, †median, or ‡frequency (%).
Median (values) and Mann–Whitney U test were used GSW, gunshot wound; IED, improvised explosive device.
to compare skewed continuous data, while median and
χ were used for ordinal data. Binary logistic regression analyses of the anatomical
2
and physiological parameters used by the US model
Binary logistic regression analysis was used to assess pa- are shown in Table 2. Sensitivity and specificity for this
rameters for their individual predictive value. The current model are shown in Table 3, along with the sensitiv-
US guidance for the use of blood products by prehospital ity and specificity for this rule with two modifications
practitioners was measured for sensitivity, specificity, and aimed at improving sensitivity.
positive and negative predictive values. Likelihood ratios
were also calculated, as they are a better measure of the Table 2 Odds Ratios and 95% CIs for Factors Used
effectiveness of a test than positive predictive value when in the US Model Predicting the Use of Acute/Massive
the prevalence of the condition varies between popula- Blood Transfusion
tions. The benefit of this test is that it can be used to com- Odds 95% CI
pare with different populations in the future. Significance Ratio Lower Upper
Based on the predetermined predictive value of other SBP <90mmHg <.001 12.636 5.42 29.462
variables, further testing of the US protocol for sensi- SBP <100mmHg <.001 14.807 7.48 29.31
8
tivity and specificity was performed in an attempt to im- Pulse ≥120/min <.001 8.422 4.322 16.409
prove the current guidance. Pulse ≥110/min <.001 6.338 3.357 11.963
Advice regarding ethical approval was sought from the Above-knee .002 7.23 2.022 25.853
amputation
Director of Research at the Royal Centre for Defence
Medicine. Ministry of Defence Research Ethics Commit- Above- or .024 4.00 1.202 13.309
below-knee
tee approval was not required as the study was identi- amputation
fied as a service evaluation and improvement program. 12
Discussion
Results
The SME consensus guidelines developed for use by
We identified 476 casualties, which represented 19.2% DUSTOFF TACEVAC assets in Afghanistan were validated
of patients presenting to the hospital during the study by this retrospective study. An injury pattern comprising
period. The mean age of these casualties was 26.76 a double above-knee amputation was highly predictive
50 Journal of Special Operations Medicine Volume 14, Edition 4/Winter 2014