
Page 54 - ATP-P 11th Ed
P. 54
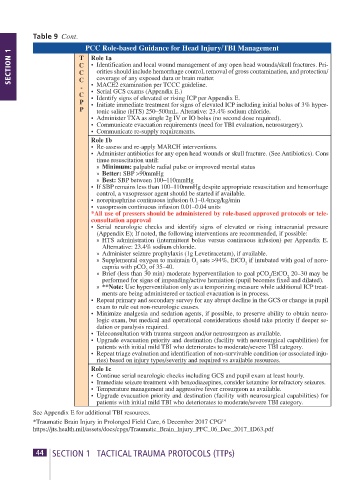
Table 9 Cont.
PCC Role-based Guidance for Head Injury/TBI Management
SECTION 1 T Role 1a
C • Identification and local wound management of any open head wounds/skull fractures. Pri-
orities should include hemorrhage control, removal of gross contamination, and protection/
C
coverage of any exposed dura or brain matter.
C
- • MACE2 examination per TCCC guideline.
C • Serial GCS exams (Appendix E.)
• Identify signs of elevated or rising ICP per Appendix E.
P • Initiate immediate treatment for signs of elevated ICP including initial bolus of 3% hyper-
P tonic saline (HTS) 250–500mL. Alterative: 23.4% sodium chloride.
• Administer TXA as single 2g IV or IO bolus (no second dose required).
• Communicate evacuation requirements (need for TBI evaluation, neurosurgery).
• Communicate re-supply requirements.
Role 1b
• Re-assess and re-apply MARCH interventions.
• Administer antibiotics for any open head wounds or skull fracture. (See Antibiotics). Cons -
tinue resuscitation until:
» Minimum: palpable radial pulse or improved mental status
» Better: SBP >90mmHg
» Best: SBP between 100–110mmHg
• If SBP remains less than 100–110mmHg despite appropriate resuscitation and hemorrhage
control, a vasopressor agent should be started if available.
• norepinephrine continuous infusion 0.1–0.4mcg/kg/min
• vasopressin continuous infusion 0.01–0.04 units
*All use of pressers should be administered by role-based approved protocols or tele-
con sul tation approval
• Serial neurologic checks and identify signs of elevated or rising intracranial pressure
( Appendix E); If noted, the following interventions are recommended, if possible:
» HTS administration (intermittent bolus versus continuous infusion) per Appendix E.
Alternative: 23.4% sodium chloride.
» Administer seizure prophylaxis (1g Levetiracetam), if available.
» Supplemental oxygen to maintain O sats >94%, EtCO if intubated with goal of noro-
capnia with pCO of 35–40. 2 2
2
» Brief (less than 30 min) moderate hyperventilation to goal pCO /EtCO 20–30 may be
2
2
performed for signs of impending/active herniation (pupil becomes fixed and dilated).
» **Note: Use hyperventilation only as a temporizing measure while additional ICP treat-
ments are being administered or tactical evacuation is in process.
• Repeat primary and secondary survey for any abrupt decline in the GCS or change in pupil
exam to rule out non-neurologic causes.
• Minimize analgesia and sedation agents, if possible, to preserve ability to obtain neuro-
logic exam, but medical and operational considerations should take priority if deeper se-
dation or paralysis required.
• Teleconsultation with trauma surgeon and/or neurosurgeon as available.
• Upgrade evacuation priority and destination (facility with neurosurgical capabilities) for
patients with initial mild TBI who deteriorates to moderate/severe TBI category.
• Repeat triage evaluation and identification of non-survivable condition (or associated inju-
ries) based on injury types/severity and required vs available resources.
Role 1c
• Continue serial neurologic checks including GCS and pupil exam at least hourly.
• Immediate seizure treatment with benzodiazepines, consider ketamine for refractory seizures.
• Temperature management and aggressive fever crosurgeon as available.
• Upgrade evacuation priority and destination (facility with neurosurgical capabilities) for
patients with initial mild TBI who deteriorates to moderate/severe TBI category.
See Appendix E for additional TBI resources.
*Traumatic Brain Injury in Prolonged Field Care, 6 December 2017 CPG 14
https://jts.health.mil/assets/docs/cpgs/Traumatic_Brain_Injury_PFC_06_Dec_2017_ID63.pdf
44 SECTION 1 TACTICAL TRAUMA PROTOCOLS (TTPs) ATP-P Handbook 11th Edition 45